IMAGING
BREAST SELF-EXAMS AND MAMMOGRAMS
BREAST SELF-EXAMS
BREAST SELF-EXAMS ARE HELPFUL!

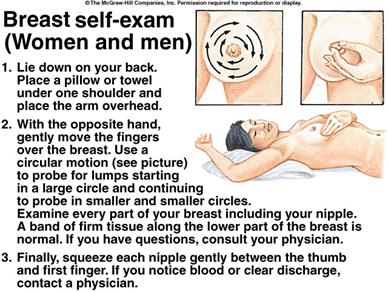
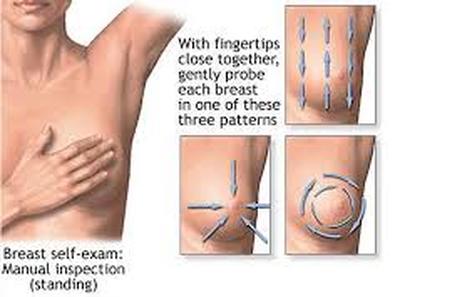
HOW TO PERFORM BREAST SELF-EXAMS
"Mammography screening is a profit-driven technology posing risks compounded by unreliability. In striking contrast, annual clinical breast examination (CBE) by a trained health professional, together with monthly breast self-examination (BSE), is safe, at least as effective, and low in cost. International programs for training nurses how to perform CBE and teach BSE are critical and overdue."
Samuel Epstein, MD, Rosalie Bertell, PHD, and Barbara Seaman, Dangers and Unreliability of Mammography: Breast Examination is a Safe, Effective, and Practical Alternative, Int J Health, 2001.
Samuel Epstein, MD, Rosalie Bertell, PHD, and Barbara Seaman, Dangers and Unreliability of Mammography: Breast Examination is a Safe, Effective, and Practical Alternative, Int J Health, 2001.
FROM DERMATOLOY NEWS:
"Residents trained using the vertical strip clinical breast exam are significantly more likely to detect and be able to describe small breast masses, Elizabeth Steiner, M.D., reported at the annual meeting of the North American Primary Care Research Group. The vertical strip, three-pressure method examines the breast in overlapping vertical strips using the pads of the first three fingers with light, then medium, then deep pressure. It covers a wide area of the chest from the clavicle down to the inframammary ridge and out to the lymph nodes.
Unlike the standard concentric circle or wedge methods, it includes the entire nipple-areolar complex where 15%–20% of breast cancers originate, said Dr. Steiner, of Oregon Health and Science University, Portland.
The method has been endorsed as the best breast exam method by the Centers for Disease Control and Prevention and the American Cancer Society (CA Cancer J. Clin. 2004;54:327–44). But it has a drawback: It takes 3–5 minutes per breast to perform.
'One of the things we get from diagnosticians is that this takes too long,”'Dr. Steiner said in an interview. 'But the one factor that has been shown to make a difference in every study about breast exam sensitivity is the time you take. In our study, for every 15 seconds you took, it made you 29% more likely to find a 3-mm mass'."
http://www.edermatologynews.com/index.php?id=1059&type=98&tx_ttnews[tt_news]=44424&cHash=da03e20e36
"Residents trained using the vertical strip clinical breast exam are significantly more likely to detect and be able to describe small breast masses, Elizabeth Steiner, M.D., reported at the annual meeting of the North American Primary Care Research Group. The vertical strip, three-pressure method examines the breast in overlapping vertical strips using the pads of the first three fingers with light, then medium, then deep pressure. It covers a wide area of the chest from the clavicle down to the inframammary ridge and out to the lymph nodes.
Unlike the standard concentric circle or wedge methods, it includes the entire nipple-areolar complex where 15%–20% of breast cancers originate, said Dr. Steiner, of Oregon Health and Science University, Portland.
The method has been endorsed as the best breast exam method by the Centers for Disease Control and Prevention and the American Cancer Society (CA Cancer J. Clin. 2004;54:327–44). But it has a drawback: It takes 3–5 minutes per breast to perform.
'One of the things we get from diagnosticians is that this takes too long,”'Dr. Steiner said in an interview. 'But the one factor that has been shown to make a difference in every study about breast exam sensitivity is the time you take. In our study, for every 15 seconds you took, it made you 29% more likely to find a 3-mm mass'."
http://www.edermatologynews.com/index.php?id=1059&type=98&tx_ttnews[tt_news]=44424&cHash=da03e20e36
BREAST IMAGING - BREAST SELF-EXAM
MAMMOGRAPHY DOES NOT REDUCE MORTALITY IN 40-59 YEARS OLD GROUP BEYOND THAT OF PHYSICAL BREAST EXAM - LET YOUR FINGERS DO THE BREAST IMAGING
"I began to feel that what the trial was showing was that clinical breast exam was effective and could substitute for mammography, if it was performed well and was accompanied by the teaching of breast self-exam."
Dr.Anthony Miller, 2014 http://well.blogs.nytimes.com/2014/02/17/a-fresh-case-for-breast-self-exams/?_r=0)
Dr.Anthony Miller, 2014 http://well.blogs.nytimes.com/2014/02/17/a-fresh-case-for-breast-self-exams/?_r=0)
In the Miller AB et al. 2014 study, the objective of the researchers was, "To compare breast cancer incidence and mortality up to 25 years in women aged 40-59 who did or did not undergo mammography screening."
In this study, 90,000 women were divided in half and given either mammograms and taught to do breast exams or, in the other half just were taught and practiced self-breast exams, and all were followed for twenty-five years.
"What is already known on this topic:
*Women with non-palpable breast cancer detected by mammography experience long term survival that is superior to that of women with palpable breast cancer
*It is not known with accuracy to what extent the survival difference is a consequence of organized screening or of lead time bias and over-diagnosis."
And now, "What this study adds:
*Annual mammography screening detected a significant number of small non-palpable breast cancers, but half of these were examples of over-diagnosis.
(See Miller AB et al., Twenty-Five Year Follow-Up for Breast Cancer Incidence and Mortality of the Canadian National Breast Screening Study: Randomized Screening Trial, BMJ, 2014.)
In this study, 90,000 women were divided in half and given either mammograms and taught to do breast exams or, in the other half just were taught and practiced self-breast exams, and all were followed for twenty-five years.
"What is already known on this topic:
*Women with non-palpable breast cancer detected by mammography experience long term survival that is superior to that of women with palpable breast cancer
*It is not known with accuracy to what extent the survival difference is a consequence of organized screening or of lead time bias and over-diagnosis."
And now, "What this study adds:
*Annual mammography screening detected a significant number of small non-palpable breast cancers, but half of these were examples of over-diagnosis.
- 22% of the screen detected invasive cancers in the mammography arm were over-diagnosed, representing one over-diagnosed breast cancer for every 424 women who received mammography screening in the trial
- Annual mammography screening had no effect on breast cancer mortality beyond that of breast physical examinations."
(See Miller AB et al., Twenty-Five Year Follow-Up for Breast Cancer Incidence and Mortality of the Canadian National Breast Screening Study: Randomized Screening Trial, BMJ, 2014.)
MAMMOGRAMS - THINKING ABOUT HAVING A ROUTINE MAMMOGRAM?
*Mammogram Debate*
BREAST IMAGING - MAMMOGRAMS

BREAST IMAGING- MAMMOGRAMS - DEFINITION
"A mammogram is an x-ray of the breast that is used to detect and evaluate breast changes.....
The x-ray machines used for mammograms today expose the breast to much less radiation that those used in the past."
(See www.cancer.org/treatment/understand-other-breast-imaging-procedures-what-is-mammogram.)
The x-ray machines used for mammograms today expose the breast to much less radiation that those used in the past."
(See www.cancer.org/treatment/understand-other-breast-imaging-procedures-what-is-mammogram.)
TYPES OF MAMMOGRAMS
"Screening mammograms involve two x-rays of each breast. Diagnostic mammograms usually are employed to check on breast aberrations, such as lumps, thickened skin, discharges, etc. Diagnostic mammograms are a more detailed exam, which involve images of the breasts from many different angles."
(See http://womenshealth.gov/publications/our-publications/fact-sheet/mammograms.html.)
"3-D ,mammograms, known as tomosynthesis, are now widely promoted. "To achieve a three-dimensional image, the machine moves in an arc around your breast, taking multiple x-rays along the way, which are then computed together into a 3D image."
Dr Joseph Mercola, 2013, http://articles.mercola.com/sites/articles/archive/2013/02/19/tomosynthesis-mammography.aspx 2013
(See http://womenshealth.gov/publications/our-publications/fact-sheet/mammograms.html.)
"3-D ,mammograms, known as tomosynthesis, are now widely promoted. "To achieve a three-dimensional image, the machine moves in an arc around your breast, taking multiple x-rays along the way, which are then computed together into a 3D image."
Dr Joseph Mercola, 2013, http://articles.mercola.com/sites/articles/archive/2013/02/19/tomosynthesis-mammography.aspx 2013
*Mammogram Debate*
WHEN TO GET A ROUTINE MAMOGRAM?
Daniel Kopans, MD, stated that for women who have had mammograms, there was more than a 30% reduction in breast cancer deaths. He wants women to start having mammograms at the age of 40, while the US Preventive Services' Task Force recommends having one every two years after the age of 50, and the Swiss Medical Board and Dr. Eric Topol wonder about the wisdom of having mammograms altogether, without any underpinning genetic or other reason to do so. .... Is it time to realize, as in the Harding C et al. 2015 study, that "the potential for over diagnosis is very high" with mammograms, and that with mammography's "diagnosis of additional small cancers", that larger tumors aren't found and deaths aren't decreased?
WHEN TO GET A ROUTINE MAMOGRAM?
Daniel Kopans, MD, stated that for women who have had mammograms, there was more than a 30% reduction in breast cancer deaths. He wants women to start having mammograms at the age of 40, while the US Preventive Services' Task Force recommends having one every two years after the age of 50, and the Swiss Medical Board and Dr. Eric Topol wonder about the wisdom of having mammograms altogether, without any underpinning genetic or other reason to do so. .... Is it time to realize, as in the Harding C et al. 2015 study, that "the potential for over diagnosis is very high" with mammograms, and that with mammography's "diagnosis of additional small cancers", that larger tumors aren't found and deaths aren't decreased?
WHEN TO GET A ROUTINE MAMMOGRAM?
AMERICAN CANCER SOCIETY - 2015 MAMMOGRAM GUIDELINES
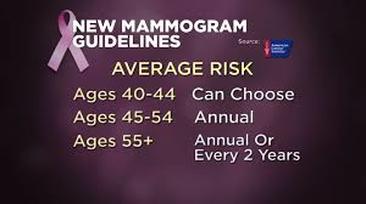
- Women ages 40 to 44 should have the choice to start annual breast cancer screening with mammograms (x-rays of the breast) if they wish to do so.
- Women age 45 to 54 should get mammograms every year.
- Women 55 and older should switch to mammograms every 2 years, or can continue yearly screening.
- Screening should continue as long as a woman is in good health and is expected to live 10 more years or longer.
- All women should be familiar with the known benefits, limitations, and potential harms linked to breast cancer screening. They also should know how their breasts normally look and feel and report any breast changes to a health care provider right away.
- (See American Cancer Societyhttp://www.cancer.org/healthy/findcancerearly/cancerscreeningguidelines/american-cancer-society-guidelines-for-the-early-detection-of-cancer.)
WHEN TO GET A ROUTINE MAMMOGRAM? TO THE CONTRARY: SWITZERLAND!
ABOLISH ROUTINE MAMMOGRAPHY SCREENING?
"It is not recommended that systemic mammograms be introduced."
(Swiss Medical Board, 2014, (www.medical-board.ch.)
(Swiss Medical Board, 2014, (www.medical-board.ch.)
In their 2014 article, Biller-Adorno N and Juni P wrote about the Swiss Medical Board's recommendation against mammograms, that "systemic mammograms" not be introduced. The Swiss Medical Board's 2014 report "acknowledged that systematic mammography screening might prevent about one death attributed to breast cancer for every 1000 women screened, even though there was no evidence to suggest that overall mortality was affected. At the same time, it emphasized the harm — in particular, false positive test results and the risk of over diagnosis.- Conclusion: " It is easy to promote mammography screening if the majority of women believe that it prevents or reduces the risk of getting breast cancer and saves many lives through early detection of aggressive tumors. We would be in favor of mammography screening if these beliefs were valid. Unfortunately, they are not, and we believe that women need to be told so. From an ethical perspective, a public health program that does not clearly produce more benefits than harms is hard to justify. Providing clear, unbiased information, promoting appropriate care, and preventing overdiagnosis and overtreatment would be a better choice."
- (See Biller-Adorno N and Juni P,Abolishing Mammogram Screening Programs? A View From the Swiss Medical Board, NEJM, 2014, http://www.nejm.org/doi/full/10.1056/NEJMp1401875.)
WHEN TO GET A ROUTINE MAMMOGRAM? STOP ROUTINE MAMMOS?
"Until now, the use of mass screening suggests that we are unable to differentiate the risk in any given individual. So instead of a smart approach that uses family history and genetics, we have dumbed it down and treated all women the same. As a result, we have come to rely on a test that is notoriously inaccurate but has become a fixed part of American medical practice since it was introduced almost 50 years ago."
Eric Topol, MD
Eric Topol, MD
- In Eric Topol, MD's Editorial in Medscape, he penned, "It is time to reboot how we screen for breast cancer. Until now, the use of mass screening suggests that we are unable to differentiate the risk in any given individual. So instead of a smart approach that uses family history and genetics, we have dumbed it down and treated all women the same. As a result, we have come to rely on a test that is notoriously inaccurate but has become a fixed part of American medical practice since it was introduced almost 50 years ago. With the tens of millions of low-risk women unnecessarily undergoing screening each year, any test would be vulnerable to a high rate of false positives. That applies to higher-resolution scans, too, such as magnetic resonance, digital mammography and ultrasound ..." (See Eric Topol, MD., Time to End Routine Mammography, Medscape,

WHEN TO GET A ROUTINE MAMMOGRAM? EVIDENCE STRONGLY SUGGESTS MAMMOGRAPHY SCREENING EACH YEAR BEGINNING AT AGE OF 40
"There are now more than 30% fewer women who die each year from breast cancer than would have died had screening not been available.."
Daniel Kopans, MD
Daniel Kopans, MD
"In the US, the death rate from breast cancer has been unchanged going back to 1940. mammography screening began in the mid-1980s at a national level, and, as predicted, the death rates began to fall for the first time in 50 years, in 1990. There are now more than 30% fewer women who die each year from breast cancer than would have died had screening not been available. ... While we work day and night to find a cure or prevention, women should be advised that the scientific evidence strongly suggests mammography screening each year beginning at the age of 40."
(Daniel Kopans, MD., Denying Women Access to Mammography Screening, Med Page, 20 http://www.medpagetoday.com/HematologyOncology/BreastCancer/48097
(Daniel Kopans, MD., Denying Women Access to Mammography Screening, Med Page, 20 http://www.medpagetoday.com/HematologyOncology/BreastCancer/48097
HOW EFFECTIVE ARE MAMMOS?

HOW EFFECTIVE ARE MAMMOGRAMS?
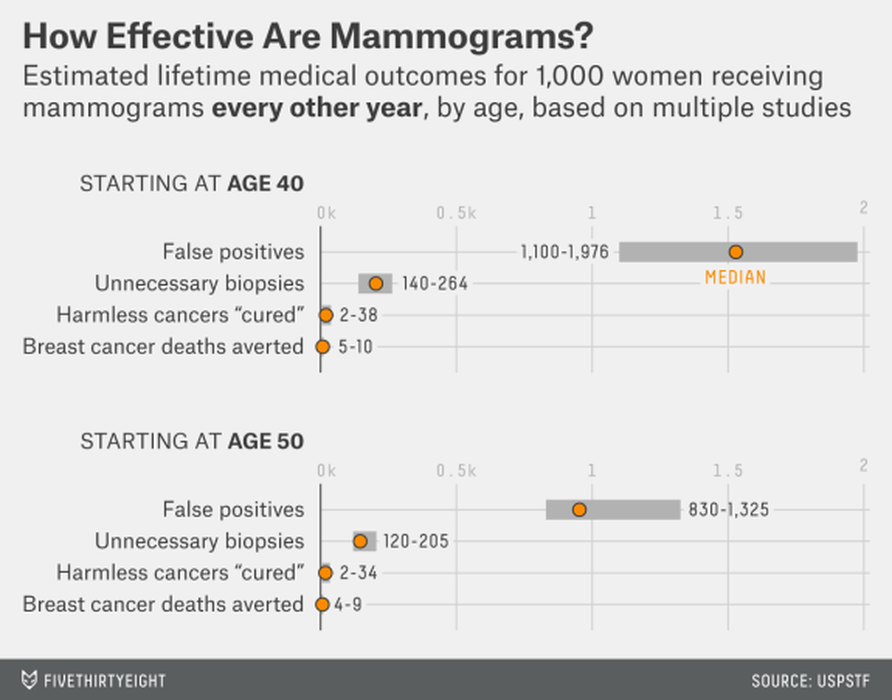
"This chart shows the likelihood of various outcomes of biennial mammograms for women starting at age 40 and at age 50, according to the US Preventive Services Task Force. 'False positives' are suspicious findings that do not turn out to be cancer."
http://fivethirtyeight.com/features/science-wont-settle-the-mammogram-deba
"This chart shows the likelihood of various outcomes of biennial mammograms for women starting at age 40 and at age 50, according to the US Preventive Services Task Force. 'False positives' are suspicious findings that do not turn out to be cancer."
http://fivethirtyeight.com/features/science-wont-settle-the-mammogram-deba
THE MAMMOGRAM DEBATE - OVER DIAGNOSIS?
The Hellquist B et al. 2010 study below found a reduction in mortality rate estimated at 26% to 29% for women aged 40-49 who had gotten mammograms. The reduction in mortality was greater for those in the 45-49 years range than for those 40-44.
But what kinds of tumors are being found with more screening?
The Harding C et al. 2015 study, also below, wondered if just "small, indolent, or regressive tumors that would not otherwise become clinically apparent" were being found on mammograms.
In an ecological study, " Counties (in the US) with the most screening had substantially more cancer being diagnosed. ... In fact, there was 1.8 times more cancer being found in the counties with more screening than in the counties with the least screening."
Small or large tumors?
More screenings were "very strong" finding small tumors. These are tumors that are less than two centimeters.
Additional small cancers were definitely found. However, " ...There is no concomitant decline in the detection of larger cancers, which might explain the absence of any significant differences in the overall rate of death from the disease. Together, these findings suggest widespread over diagnosis." READ STUDIES BELOW.
The Hellquist B et al. 2010 study below found a reduction in mortality rate estimated at 26% to 29% for women aged 40-49 who had gotten mammograms. The reduction in mortality was greater for those in the 45-49 years range than for those 40-44.
But what kinds of tumors are being found with more screening?
The Harding C et al. 2015 study, also below, wondered if just "small, indolent, or regressive tumors that would not otherwise become clinically apparent" were being found on mammograms.
In an ecological study, " Counties (in the US) with the most screening had substantially more cancer being diagnosed. ... In fact, there was 1.8 times more cancer being found in the counties with more screening than in the counties with the least screening."
Small or large tumors?
More screenings were "very strong" finding small tumors. These are tumors that are less than two centimeters.
Additional small cancers were definitely found. However, " ...There is no concomitant decline in the detection of larger cancers, which might explain the absence of any significant differences in the overall rate of death from the disease. Together, these findings suggest widespread over diagnosis." READ STUDIES BELOW.
BREAST IMAGING - MAMMOGRAMS
MAMMOGRAM BENEFITS FOR 40-49 YEARS OLD GROUP? DEATH RATE AROUND 29% LOWER IN WOMEN WHO GOT MAMMOGRAMS. BENEFITS HIGHER AGES 45-49 THAN 40-44.
In 2010, Hellquist B et al. conducted a retrospective study on mammograms and mortality in Sweden on women from the ages of 40-49.
This study was on this young cohort of women, from the years 1986 to 2005, who either had gotten their mammograms or did not do any screening.
Results: "During the study period, there were 803 breast cancer deaths in the study group (7.3 million person-years) and 1238 breast cancer deaths in the control group (8.8 million person-years)."
Conclusion: "...The current large study of the Swedish service-screening program with mammography for women ages 40 to 49 revealed a reduction in breast cancer mortality. The reduction was estimated at 26% to 29%, depending on the studied exposure. The reduction was greater only when those women who actually attended screening were considered, and it also was greater among women ages 45 to 49 years than among women ages 40 to 44 years."
(See Hellquist B et al., Effectiveness of Population-Based Service Screening with Mammography on Women Ages 40-49 Years, Cancer, 2010.)
BREAST IMAGING - MAMMOGRAMS - MORE SCREENING FINDS SMALLER TUMORS WITH NO DECREASE IN BREAST CANCER DEATHS.
NEWLY DIAGNOSED WITH BREAST CANCER AFTER A MAMMOGRAM? COULD IT JUST BE AN OVER DIAGNOSIS?
Maybe so! ......... According to Charles Harding, the "potential for overdiagnosis is very high".
The 2015 JAMA Press Release on the Harding C et al. 2015 study stated, "...There are increasing concerns that screening (mammography) unintentionally leads to overdiagnosis by identifying small, indolent, or regressive tumors that would not otherwise become clinically apparent."
In the Harding C et al. 2015 study, the researchers "conducted an ecological study of 16 million women ages 40 and older who lived in 547 counties reporting to Surveillance, Epidemiology and End Results cancer registries during the year 2000. Of these women, 53,207 were diagnosed with breast cancer that year and followed up for the next 10 years. The authors examined the extent of screening in each county and measured breast cancer incidence in 2000 and incidence-based breast cancer death during the 10-year follow-up, with incidence and mortality calculated for each county." Findings: Researcher Charles Harding commented on JAMA media net, " Counties (in the US) with the most screening had substantially more cancer being diagnosed. ... In fact, there was 1.8 times more cancer being found in the counties with more screening than in the counties with the least screening."
Were these additional cancer tumors being found large tumors or small tumors?
Researcher Charles Harding commented that more screenings were "very strong" for small tumors. These are tumors that are less than two centimeters. Indeed, these smaller tumors were more than twice times (2.2 times) found in the more highly screened group. For the larger tumors, there was very little difference.
But, while there may be "a correlation between the extent of screening and breast cancer incidence", is there a correlation with breast cancer deaths?
Researcher Charles Harding commented, "We did not find significant changes in breast cancer deaths in the counties with the most screening. ... This was surprising to me, since breast cancer is a leading cause of death."
Conclusion from the study: "When analyzed at the county level, the clearest result of mammography screening is the diagnosis of additional small cancers. Furthermore, there is no concomitant decline in the detection of larger cancers, which might explain the absence of any significant differences in the overall rate of death from the disease. Together, these findings suggest widespread overdiagnosis."
Limitations of study; This was an ecological study, which studies groups, not individuals, making it hard to extrapolate what happened on an individual basis. Drs. Joann Elmore and Ruth Etzioni observed, “However, much has also been written about the caution needed when interpreting ecological analyses. It is well known, for example, that ecological studies provide no information as to whether the people who were actually exposed to the intervention were the same people who developed the disease, whether the exposure or the onset of disease came first, or whether there are other explanations for the observed association."
(For the JAMA Press Release along with the Charles Harding and Dr. Joann Elmore commentary,, see http: //media.jamanetwork.com/news-item/detecting-more-small-cancers-in-screening-mammography-suggests-overdiagnosis/. For the study, see Harding C et al., Breast Cancer Screening Incidence and Mortality Across US Counties, JAMA, 2015.)
The 2015 JAMA Press Release on the Harding C et al. 2015 study stated, "...There are increasing concerns that screening (mammography) unintentionally leads to overdiagnosis by identifying small, indolent, or regressive tumors that would not otherwise become clinically apparent."
In the Harding C et al. 2015 study, the researchers "conducted an ecological study of 16 million women ages 40 and older who lived in 547 counties reporting to Surveillance, Epidemiology and End Results cancer registries during the year 2000. Of these women, 53,207 were diagnosed with breast cancer that year and followed up for the next 10 years. The authors examined the extent of screening in each county and measured breast cancer incidence in 2000 and incidence-based breast cancer death during the 10-year follow-up, with incidence and mortality calculated for each county." Findings: Researcher Charles Harding commented on JAMA media net, " Counties (in the US) with the most screening had substantially more cancer being diagnosed. ... In fact, there was 1.8 times more cancer being found in the counties with more screening than in the counties with the least screening."
Were these additional cancer tumors being found large tumors or small tumors?
Researcher Charles Harding commented that more screenings were "very strong" for small tumors. These are tumors that are less than two centimeters. Indeed, these smaller tumors were more than twice times (2.2 times) found in the more highly screened group. For the larger tumors, there was very little difference.
But, while there may be "a correlation between the extent of screening and breast cancer incidence", is there a correlation with breast cancer deaths?
Researcher Charles Harding commented, "We did not find significant changes in breast cancer deaths in the counties with the most screening. ... This was surprising to me, since breast cancer is a leading cause of death."
Conclusion from the study: "When analyzed at the county level, the clearest result of mammography screening is the diagnosis of additional small cancers. Furthermore, there is no concomitant decline in the detection of larger cancers, which might explain the absence of any significant differences in the overall rate of death from the disease. Together, these findings suggest widespread overdiagnosis."
Limitations of study; This was an ecological study, which studies groups, not individuals, making it hard to extrapolate what happened on an individual basis. Drs. Joann Elmore and Ruth Etzioni observed, “However, much has also been written about the caution needed when interpreting ecological analyses. It is well known, for example, that ecological studies provide no information as to whether the people who were actually exposed to the intervention were the same people who developed the disease, whether the exposure or the onset of disease came first, or whether there are other explanations for the observed association."
(For the JAMA Press Release along with the Charles Harding and Dr. Joann Elmore commentary,, see http: //media.jamanetwork.com/news-item/detecting-more-small-cancers-in-screening-mammography-suggests-overdiagnosis/. For the study, see Harding C et al., Breast Cancer Screening Incidence and Mortality Across US Counties, JAMA, 2015.)
BREAST IMAGING - MAMMOGRAMS - HARM? DO MAMMOGRAMS CAUSE ANY DNA AND CHROMOSOME DAMAGE IN LYMPHOCYTES?
"Our results indicate that exposure to mammography X-rays resulted in a modest increase in the induction of double strand breaks compared to γ (gamma)-rays. However, due to the higher linear energy transfer of mammography X-rays more clustered DNA damage is produced that is more difficult to repair and results in a more pronounced increase in micronucleus formation."
Depuydt J et al., 2013
Depuydt J et al., 2013
Yes!
In the Depuydt J et al. 2013 study, the researchers investigated the "benefit/risk ratio" of mammograms at the "level of DNA and chromosomes in lymphocytes".
Blood, derived from healthy women, was "irradiated in vitro with 30 kV X-rays and (60)Co γ-rays with doses between 5 and 2000 mGy."
Conclusion: "Our results indicate that exposure to mammography X-rays resulted in a modest increase in the induction of double strand breaks compared to γ (gamma)-rays. However, due to the higher linear energy transfer of mammography X-rays more clustered DNA damage is produced that is more difficult to repair and results in a more pronounced increase in micronucleus formation."
(See Depuydt J et al., Relative Biological Effectiveness of Mammography X-Rays at the Level of DNA and Chromosomes in Lymphocytes, Int J Radiat Biol, 2013.)
Yes!
In the Depuydt J et al. 2013 study, the researchers investigated the "benefit/risk ratio" of mammograms at the "level of DNA and chromosomes in lymphocytes".
Blood, derived from healthy women, was "irradiated in vitro with 30 kV X-rays and (60)Co γ-rays with doses between 5 and 2000 mGy."
Conclusion: "Our results indicate that exposure to mammography X-rays resulted in a modest increase in the induction of double strand breaks compared to γ (gamma)-rays. However, due to the higher linear energy transfer of mammography X-rays more clustered DNA damage is produced that is more difficult to repair and results in a more pronounced increase in micronucleus formation."
(See Depuydt J et al., Relative Biological Effectiveness of Mammography X-Rays at the Level of DNA and Chromosomes in Lymphocytes, Int J Radiat Biol, 2013.)
THINKING ABOUT 3-D MAMMOGRAPHY?

CONSIDERING 3-D MAMMOGRAMS?
BENEFITS
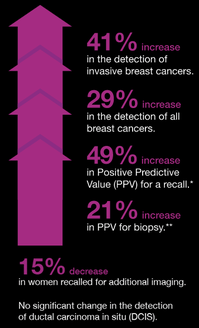
*41% increase in detection of invasive breast cancers
*29% increase in detection of all cancers
*49% increase in Positive Predictive Value for a recall.
*29% increase in Positive Predictive Value for biopsy.
"The addition of tomosynthesis to digital mammography was associated with a decrease in the recall rate and an increase in cancer detection."
Friedewald SM et al., 2014.
BENEFITS
*41% increase in detection of invasive breast cancers
*29% increase in detection of all cancers
*49% increase in Positive Predictive Value for a recall.
*29% increase in Positive Predictive Value for biopsy.
"The addition of tomosynthesis to digital mammography was associated with a decrease in the recall rate and an increase in cancer detection."
Friedewald SM et al., 2014.
CONSIDERING 3-D MAMMOGRAMS?
HARM
Excerpts from Dr. Mercola:
* "Since the 3D mammogram requires multiple views in order to achieve three-dimensionality, it stands to reason your total radiation dose from 3D mammography can be considerably higher than a standard 2D mammogram.
*We know all levels of ionizing radiation can cause cancer but, astonishingly, radiologists still want you to have your traditional mammogram screening first, followed by a 3D tomosynthesis mammogram for those with dense breasts or an area of suspicion!
* Again, this is not progress — it's a huge step backward, making cancer screening even more dangerous than before.
* Granted, a study.... (which included more than 12,600 women), showed a 40 percent increase in the detection or identification of invasive cancers, and a 15 percent decrease in false positives when adding 3D mammography to traditional 2D screening. But while this sounds good, this must be weighed against the now significantly increased risk of the test itself CAUSING fatal cancer."
Dr. Joseph Mercola, 2013.http://articles.mercola.com/sites/articles/archive/2013/02/19/tomosynthesis-mammography.aspx 2013,
BREAST IMAGING - MAMMOGRAMS - HARM VS. BENEFITS FROM 3-D MAMMOS (TOMOSYNTHESIS)
TOMOSYNTHESIS 1.5 to 2 TIMES RADIATION DOSE OF MAMMOGRAMS, FDA FOUND DOUBLE THE DOSE, RADIOLOGISTS REPORT TRIPLE THE RADIATION DOSE.

From Dr. Joseph Mercola: "The 3D mammogram (tomosynthesis) requires multiple views in order to achieve three-dimensionality, so it stands to reason your total radiation exposure would be considerably higher than from a standard 2D mammogram.
With mammography, each breast is X-rayed at least twice—once from top to bottom and once diagonally from the outside in. With tomosynthesis, the X-ray tube rotates around the breast. Twenty-five exposures are taken, with up to two pictures per second. Multiple images result in higher radiation exposure. But the picture gets even worse...
3D mammography is not a stand-alone diagnostic test—it’s typically an add-on to the standard mammogram. So, not only do these 3D images prolong your exposure to radiation, but if you’ve already had a regular mammogram, they further compound your risk. This is certainly NOT progress—it’s a huge step backward, making breast cancer screening even more dangerous than before." (See Dr. Joseph Mercola, 2013,http://articles.mercola.com/sites/articles/archive/2013/08/27/3d-mammogram-risks.aspx.)
With mammography, each breast is X-rayed at least twice—once from top to bottom and once diagonally from the outside in. With tomosynthesis, the X-ray tube rotates around the breast. Twenty-five exposures are taken, with up to two pictures per second. Multiple images result in higher radiation exposure. But the picture gets even worse...
3D mammography is not a stand-alone diagnostic test—it’s typically an add-on to the standard mammogram. So, not only do these 3D images prolong your exposure to radiation, but if you’ve already had a regular mammogram, they further compound your risk. This is certainly NOT progress—it’s a huge step backward, making breast cancer screening even more dangerous than before." (See Dr. Joseph Mercola, 2013,http://articles.mercola.com/sites/articles/archive/2013/08/27/3d-mammogram-risks.aspx.)
BREAST IMAGING - MAMMOGRAMS - HARM VS. BENEFITS FROM 3-D MAMMOS (TOMOSYNTHESIS)?
RISKS, YES, IN RADIATION FROM TOMOSYNTHESIS. HOW ABOUT BENEFITS??
TOMOSYNTHESIS (3D MAMMOGRAMS) COMBINED WITH MAMMOGRAMS - RELATIVE INCREASE IN INVASIVE CANCER DETECTION RATE OF 41%, DECREASE IN RECALL RATE
In the Friedewald SM et al. 2014 study, the researchers conducted a retrospective study on mammograms and tomosynthesis (3D imaging), to "report the rate of screen-detected cancers and proportion of recalls per 1000 screens before and after tomosynthesis implementation".
The researchers reviewed the results from 13 breast centers for more than two years from March 2010 to December 2012 relative to the number of recall numbers and cancers found in light of using tomosynthesis.
Results: "After implementation of tomosynthesis, the invasive cancer detection rate increased from 2.9 to 4.1 per 1000, a relative increase of 41%, while detection of DCIS was unchanged at 1.4 per 1000. The success of mammographic screening in reducing mortality is predicated on the principle of detecting and treating small, asymptomatic cancers before they have metastasized. Accordingly, the preferential increase in invasive cancer detection with addition of tomosynthesis may be of particular value to optimizing patient outcomes from mammographic screening." In addition, there was, "A reduction in recall rate of 16 per 1000 (relative decrease of 15%) was observed across the cohort screened with tomosynthesis."
Conclusion: "The addition of tomosythesis to digital mammography was associated with a decrease in recall rate and an increase in cancer detection rate. Further studies are needed to assess the relationship to clinical outcomes." (See Friedewald SM et al., Breast Cancer Screening Using Tomosynthesis in Combination With Digital Mammography, JAMA, 2014.)
The researchers reviewed the results from 13 breast centers for more than two years from March 2010 to December 2012 relative to the number of recall numbers and cancers found in light of using tomosynthesis.
Results: "After implementation of tomosynthesis, the invasive cancer detection rate increased from 2.9 to 4.1 per 1000, a relative increase of 41%, while detection of DCIS was unchanged at 1.4 per 1000. The success of mammographic screening in reducing mortality is predicated on the principle of detecting and treating small, asymptomatic cancers before they have metastasized. Accordingly, the preferential increase in invasive cancer detection with addition of tomosynthesis may be of particular value to optimizing patient outcomes from mammographic screening." In addition, there was, "A reduction in recall rate of 16 per 1000 (relative decrease of 15%) was observed across the cohort screened with tomosynthesis."
Conclusion: "The addition of tomosythesis to digital mammography was associated with a decrease in recall rate and an increase in cancer detection rate. Further studies are needed to assess the relationship to clinical outcomes." (See Friedewald SM et al., Breast Cancer Screening Using Tomosynthesis in Combination With Digital Mammography, JAMA, 2014.)
BREAST IMAGING - MAMMOGRAMS - HARM?
FALSE-POSITIVES - LONG-TERM PSYCHOLOGICAL CONSEQUENCES
In the 2013 Broderson J et al. study, the researchers recruited women who had both false and true findings on mammograms, plus women who had normal results on their mammograms, to assess psychological harms.
In their study, "The participants were asked to complete the Consequences of Screening in Breast Cancer—a validated questionnaire encompassing 12 psychosocial outcomes—at baseline, 1, 6, 18, and 36 months."
Results: "Six months after final diagnosis, women with false-positive findings reported changes in existential values and inner calmness as great as those reported by women with a diagnosis of breast cancer. Three years after being declared free of cancer, women with false-positive results consistently reported greater negative psychosocial consequences compared with women who had normal findings in all 12 psychosocial outcomes."
Conclusion: "False-positive findings on screening mammography causes long-term psychosocial harm. Three years after a false-positive finding, women experience psychosocial consequences that range between those experienced by women with a normal mammogram and those with a diagnosis of breast cancer."
(See Broderson J et al., Long-Term Psychosocial Consequences of False-Positive Screening Mammography,Ann Fam Med, 2013.)