SELF-HELP
DENTAL ISSUES AND METALS
JANUARY 2020
MERCURY AND OTHER TOXIC METALS FOUND IN NORMAL BREAST LOBULES IN MORE THAN HALF OF MASTECTOMY SAMPLES THAT CONTAINED AN INVASIVE CARCINOMA
(NOTE: By weight, amalgams contain 50% toxic mercury.)
FROM THE STUDY: "Exposure to toxic metals such as mercury has been proposed to be a risk factor for the development of breast cancer since some metals can promote genetic mutations and epigenetic changes. We sought to find what toxic metals are present in normal breast tissue and in the tumours of women who had mastectomies for invasive ductal breast carcinoma."
CONCLUSION: "Mercury was present in normal breast lobules in more than half of mastectomy samples that contained an invasive carcinoma, and in a smaller proportion of carcinomas and ductal carcinomas in situ. Other toxic metals that may interact synergistically with mercury could be detected in some samples. These findings do not provide direct evidence that toxic metals such as mercury play a role in the pathogenesis of breast cancer, but suggest that future molecular biological investigations on the role of toxic metals in breast cancer are warranted."
(See Pamphlett R et al., Elemental bioimaging shows mercury and other toxic metals in normal breast tissue and in breast cancers, PLOS ONE, January 20220.)
MERCURY AND OTHER TOXIC METALS FOUND IN NORMAL BREAST LOBULES IN MORE THAN HALF OF MASTECTOMY SAMPLES THAT CONTAINED AN INVASIVE CARCINOMA
(NOTE: By weight, amalgams contain 50% toxic mercury.)
FROM THE STUDY: "Exposure to toxic metals such as mercury has been proposed to be a risk factor for the development of breast cancer since some metals can promote genetic mutations and epigenetic changes. We sought to find what toxic metals are present in normal breast tissue and in the tumours of women who had mastectomies for invasive ductal breast carcinoma."
CONCLUSION: "Mercury was present in normal breast lobules in more than half of mastectomy samples that contained an invasive carcinoma, and in a smaller proportion of carcinomas and ductal carcinomas in situ. Other toxic metals that may interact synergistically with mercury could be detected in some samples. These findings do not provide direct evidence that toxic metals such as mercury play a role in the pathogenesis of breast cancer, but suggest that future molecular biological investigations on the role of toxic metals in breast cancer are warranted."
(See Pamphlett R et al., Elemental bioimaging shows mercury and other toxic metals in normal breast tissue and in breast cancers, PLOS ONE, January 20220.)
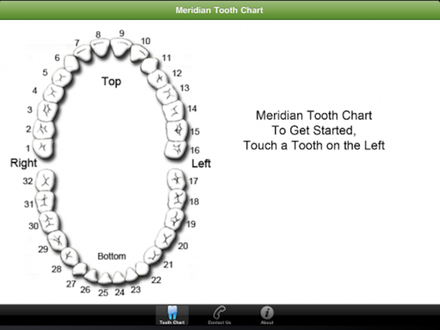
BREAST MERIDIAN CONNECTED TO TEETH #2, #3, #14, #15,# 20,# 21,# 28, #29.
CONNECTION TO THE 4th AND 5th TOOTH FROM CENTER TOOTH, RIGHT AND LEFT, UPPER AND LOWER JAW.
CONNECTION TO THE 4th AND 5th TOOTH FROM CENTER TOOTH, RIGHT AND LEFT, UPPER AND LOWER JAW.
SEEK A BIOLOGICAL DENTIST TO EVALUATE DENTAL
PROBLEMS AND REMEDIES FOR YOU TO CONSIDER
EDITORS' NOTE
While breast cancer patients are faced with making many difficult choices about their treatment strategies, dental work is arguably the greatest challenge.
TO HELP YOU WITH YOUR DENTAL ISSUES, WE URGE YOU TO SEE A BIOLOGICAL DENTIST FOR AN EVALUATION OF YOUR TEETH.
As there is a link between infected teeth and medical problems, it is incumbent upon all breast cancer patients to check out a dental meridian chart to see if they have root canals or infected teeth that lie on the meridian between the tooth and the mammary gland. Here is another helpful chart: http://iaomt.org/find-a-doctor/tooth-meridian-chart
IF YOU HAVE ROOT CANALS, AMALGAMS, OR INFECTED TEETH ON THE MERIDIAN, OR ANYWHERE ELSE IN YOUR MOUTH, IF YOU DECIDE TO HAVE A ROOT CANAL EXTRACTION, MAKE SURE THAT THE PERIODONTAL LIGAMENT IS REMOVED, AND IF YOU NEED TO HAVE AN AMALGAM REMOVED AND REFILLED OR EXTRACTED, THAT SAFETY PRECAUTIONS ARE TAKEN. A BIOLOGICAL DENTIST WILL HELP GUIDE YOU IN YOUR DECISION-MAKING PROCESS, AND DO MAKE SURE THAT ALL THE DENTAL MATERIALS ARE COMPATIBLE FOR YOU
PROBLEMS AND REMEDIES FOR YOU TO CONSIDER
EDITORS' NOTE
While breast cancer patients are faced with making many difficult choices about their treatment strategies, dental work is arguably the greatest challenge.
TO HELP YOU WITH YOUR DENTAL ISSUES, WE URGE YOU TO SEE A BIOLOGICAL DENTIST FOR AN EVALUATION OF YOUR TEETH.
As there is a link between infected teeth and medical problems, it is incumbent upon all breast cancer patients to check out a dental meridian chart to see if they have root canals or infected teeth that lie on the meridian between the tooth and the mammary gland. Here is another helpful chart: http://iaomt.org/find-a-doctor/tooth-meridian-chart
IF YOU HAVE ROOT CANALS, AMALGAMS, OR INFECTED TEETH ON THE MERIDIAN, OR ANYWHERE ELSE IN YOUR MOUTH, IF YOU DECIDE TO HAVE A ROOT CANAL EXTRACTION, MAKE SURE THAT THE PERIODONTAL LIGAMENT IS REMOVED, AND IF YOU NEED TO HAVE AN AMALGAM REMOVED AND REFILLED OR EXTRACTED, THAT SAFETY PRECAUTIONS ARE TAKEN. A BIOLOGICAL DENTIST WILL HELP GUIDE YOU IN YOUR DECISION-MAKING PROCESS, AND DO MAKE SURE THAT ALL THE DENTAL MATERIALS ARE COMPATIBLE FOR YOU
"A survey conducted at my clinic found that, on admission, ninety-eight percent of the adult cancer patients had between two and ten dead teeth, each one a dangerous toxin producing 'factory'."
Joseph Issels, MD., www.issels.com/publications/FocusOnFoci.)
PLUS, ROOT CANALS AND BACTERIA
P. acnes and Breast Cancer
P. acnes and Breast Cancer
“A compelling number of studies have documented the crucial role of some oral cavity-occurring microbes in the initiation and progression of cancers.”
https://pubmed.ncbi.nlm.nih.gov/33114460/
Bacteria Residing at Root Canals Can Induce Cell Proliferation and Alter the Mechanical Properties of Gingival and Cancer Cells
Understanding the importance of oral microbiota in human health and disease also leads to an expansion of the knowledge on functional, metabolic, and molecular alterations directly contributing to oral and systemic pathologies. To date, a compelling number of studies have documented the crucial role of some oral cavity-occurring microbes in the initiation and progression of cancers. Although this effect was noted primarily for Fusobacterium spp., the potential impact of other oral microbes is also worthy of investigation. In this study, we aimed to assess the effect of Enterococcus faecalis, Actinomyces odontolyticus, and Propionibacterium acnes on the proliferation capability and mechanical features of gingival cells and cell lines derived from lung, breast, and ovarian cancers. For this purpose, we incubated selected cell lines with heat-inactivated bacteria and supernatants collected from biofilms, cultured in both anaerobic and aerobic conditions, in the presence of surgically removed teeth and human saliva. The effect of oral bacteria on cell population growth is variable, with the highest growth-promoting abilities observed for E. faecalis in relation to human primary gingival fibroblasts (HGF) and lung cancer A549 cells, and P. acnes in relation to breast cancer MCF-7 and ovarian cancer SKOV-3 cells. Notably, this effect seems to depend on a delicate balance between the pro-stimulatory and toxic effects of bacterial-derived products. Regardless of the diverse effect of bacterial products on cellular proliferation capability, we observed significant alterations in stiffness of gingival and lung cancer cells stimulated with E. faecalis bacteria and corresponding biofilm supernatants, suggesting a novel molecular mechanism involved in the pathogenesis of diseases in oral cavities and tooth tissues. Accordingly, it is proposed that analysis of cancerogenic features of oral cavity bacteria should be multivariable and should include investigation of potential alterations in cell mechanical properties. These findings corroborate the important role of oral hygiene and root canal treatment to assure the healthy stage of oral microbiota.
(Bacteria Residing at Root Canals Can Induce Cell Proliferation and Alter the Mechanical Properties of Gingival and Cancer Cells, Suprewicz E et al., Int J Mol Sci, 2020 )
https://pubmed.ncbi.nlm.nih.gov/33114460/
Bacteria Residing at Root Canals Can Induce Cell Proliferation and Alter the Mechanical Properties of Gingival and Cancer Cells
Understanding the importance of oral microbiota in human health and disease also leads to an expansion of the knowledge on functional, metabolic, and molecular alterations directly contributing to oral and systemic pathologies. To date, a compelling number of studies have documented the crucial role of some oral cavity-occurring microbes in the initiation and progression of cancers. Although this effect was noted primarily for Fusobacterium spp., the potential impact of other oral microbes is also worthy of investigation. In this study, we aimed to assess the effect of Enterococcus faecalis, Actinomyces odontolyticus, and Propionibacterium acnes on the proliferation capability and mechanical features of gingival cells and cell lines derived from lung, breast, and ovarian cancers. For this purpose, we incubated selected cell lines with heat-inactivated bacteria and supernatants collected from biofilms, cultured in both anaerobic and aerobic conditions, in the presence of surgically removed teeth and human saliva. The effect of oral bacteria on cell population growth is variable, with the highest growth-promoting abilities observed for E. faecalis in relation to human primary gingival fibroblasts (HGF) and lung cancer A549 cells, and P. acnes in relation to breast cancer MCF-7 and ovarian cancer SKOV-3 cells. Notably, this effect seems to depend on a delicate balance between the pro-stimulatory and toxic effects of bacterial-derived products. Regardless of the diverse effect of bacterial products on cellular proliferation capability, we observed significant alterations in stiffness of gingival and lung cancer cells stimulated with E. faecalis bacteria and corresponding biofilm supernatants, suggesting a novel molecular mechanism involved in the pathogenesis of diseases in oral cavities and tooth tissues. Accordingly, it is proposed that analysis of cancerogenic features of oral cavity bacteria should be multivariable and should include investigation of potential alterations in cell mechanical properties. These findings corroborate the important role of oral hygiene and root canal treatment to assure the healthy stage of oral microbiota.
(Bacteria Residing at Root Canals Can Induce Cell Proliferation and Alter the Mechanical Properties of Gingival and Cancer Cells, Suprewicz E et al., Int J Mol Sci, 2020 )
Nov. 2019 STUDY: HAVE GUM DISEASE? " ... ORAL MICROBES CAN MEDIATE CHRONIC INFLAMMATION AND AFFECT ALL STAGES OF TUMOR DEVELOPMENT."
In the 2019 Cheng R et al. study, in a mouse model of periodontal inflammation, the periodontal inflammation was found to "promote lymph node micrometastasis, as well as head and neck metastasis of 4T1 breast cancer cells, both in early and late stages of cancer progression."
The study "demonstrated a direct link between chronic periodontal inflammation and a significant breast cancer metastatic risk. The metastatic niche formed by the gingival fibroblasts (connective tissue cells that produce collagen) was capable of recruiting macrophage, cancer epithelia, and MDSC (myeloid tumor suppressor cells are immune cells that increase during infection). ... The early steps of periodontal inflammation seem to be controlled by IL-1β (Interleukin 1 Beta proinflammatory cytokines) and macrophages in establishing a metastatic niche, whereas in presence of the tumor and MDSC cells in a later metastatic phase support tumor expansion."
CONCLUSION: "In breast cancer, IL-1β production is associated with higher rate of recurrence and is critical for tumor proliferation, angiogenesis, migration, and invasion. Our study demonstrated a direct link between chronic periodontal inflammation and a significant breast cancer metastatic risk. The metastatic niche formed by the gingival fibroblasts was capable of recruiting macrophage, cancer epithelia, and MDSC. Accordingly, inflammasome inhibitors have been proposed to limit tumor progression. ... However, this study demonstrates such a therapeutic strategy of inflammasome activity would have limited efficacy as a single agent. But, interventions for periodontitis can be considered an effectual preventative for breast cancer metastasis to the head and neck region."
(See Cheng R et al., Periodontal Inflammation Recruits Distant Metastatic Breast Cancer Cells by Increasing Myeloid-Derived Suppressor Cells, Oncogene, 2019.)
In the 2019 Cheng R et al. study, in a mouse model of periodontal inflammation, the periodontal inflammation was found to "promote lymph node micrometastasis, as well as head and neck metastasis of 4T1 breast cancer cells, both in early and late stages of cancer progression."
The study "demonstrated a direct link between chronic periodontal inflammation and a significant breast cancer metastatic risk. The metastatic niche formed by the gingival fibroblasts (connective tissue cells that produce collagen) was capable of recruiting macrophage, cancer epithelia, and MDSC (myeloid tumor suppressor cells are immune cells that increase during infection). ... The early steps of periodontal inflammation seem to be controlled by IL-1β (Interleukin 1 Beta proinflammatory cytokines) and macrophages in establishing a metastatic niche, whereas in presence of the tumor and MDSC cells in a later metastatic phase support tumor expansion."
CONCLUSION: "In breast cancer, IL-1β production is associated with higher rate of recurrence and is critical for tumor proliferation, angiogenesis, migration, and invasion. Our study demonstrated a direct link between chronic periodontal inflammation and a significant breast cancer metastatic risk. The metastatic niche formed by the gingival fibroblasts was capable of recruiting macrophage, cancer epithelia, and MDSC. Accordingly, inflammasome inhibitors have been proposed to limit tumor progression. ... However, this study demonstrates such a therapeutic strategy of inflammasome activity would have limited efficacy as a single agent. But, interventions for periodontitis can be considered an effectual preventative for breast cancer metastasis to the head and neck region."
(See Cheng R et al., Periodontal Inflammation Recruits Distant Metastatic Breast Cancer Cells by Increasing Myeloid-Derived Suppressor Cells, Oncogene, 2019.)
2019 Study: Chronic Inflammation May Link Periodontitis and Cancer
"Chronic inflammation has also been associated with several systemic diseases, like cancer. The literature demonstrates that either inflammatory mediators produced during periodontitis development could mediate carcinogenesis or periodontal bacteria can exert its effect directly in transforming cells. Interestingly, several oral bacteria, also found in high loads in the periodontal pocket, have been shown to activate inflammatory pathways associated with several stages of cellular transformation ..... Among them, these bacteria can induce NF-κB-mediated responses, promote cell survival, activate oncogenic pathways, reduce proapoptotic proteins expression, increase cell migration and invasion, increase the expression of EMT-associated proteins, enhance metastasis, etc."
(See Hoare A et al., Chronic Inflammation as a Link Between Periodontitis and Carcinogenesis, Hindawai, doi.org/10.1155/2019/1029857.)
"Chronic inflammation has also been associated with several systemic diseases, like cancer. The literature demonstrates that either inflammatory mediators produced during periodontitis development could mediate carcinogenesis or periodontal bacteria can exert its effect directly in transforming cells. Interestingly, several oral bacteria, also found in high loads in the periodontal pocket, have been shown to activate inflammatory pathways associated with several stages of cellular transformation ..... Among them, these bacteria can induce NF-κB-mediated responses, promote cell survival, activate oncogenic pathways, reduce proapoptotic proteins expression, increase cell migration and invasion, increase the expression of EMT-associated proteins, enhance metastasis, etc."
(See Hoare A et al., Chronic Inflammation as a Link Between Periodontitis and Carcinogenesis, Hindawai, doi.org/10.1155/2019/1029857.)
DENTAL ISSUES, METALS,
AND BREAST CANCER
DENTAL METALS
By weight, amalgams contain 50% toxic mercury. One of the Editors had just one amalgam tested, and after thirty years, it still tests high for mercury.
Dental amalgams harbor silver, tin, and copper. Approximately 50% of dental amalgam is elemental mercury by weight. But, through resonance testing, Hulda Clark, PHD, detected 50 metals in a single sample of new amalgam about to be placed in a patient's mouth. She found that, "Amalgam is producing a steady flow of mercury and thallium into our bodies, not to mention nickel, chromium, copper, and dozens more. ... Notice the lanthanides in amalgam: Ce, Dy, Eu, Gd, Ho, La, NO, Nb, Pr, Sm, Tb, Yb, Y. They are nearly all represented. As they diffuse out into our bodies, will their paramagnetic nature upset the delicate iron balance, will they be excretable?" And gold? Gold is hardened by nickel. "Even gold is extremely harmful, being an essential element for prions, Salmonella bacteria, SV40 virus, and even the HIV virus." (See Hulda Clark, PHD, Pages 328-329, The Prevention of All Cancers, New Century Press, 2004.)
In addition to mercury, amalgams contain a mixture of many other dangerous metals, and one independent researcher stated that 50% of amalgams may even be radioactive.
2015 REVIEW STUDY - METALLOESTROGENS, SUCH AS CADMIUM, MIMIC ESTROGEN BEING USED IN NANOPARTICLE PRODUCTION. CADMIUM, ALTHOUGH NOT BEING CAUSATIVE FOR BREAST CANCER, IS A RISK FACTOR
WHERE IS WISDOM IN USING METALLOESTROGENS FOR METALLIC FOUNDATION FOR NANOPARTICLE PRODUCTION IN CONSUMER PRODUCTS?
In his 2015 review study, David Wallace "focused on exposure to highly toxic metals, ('metalloestrogens' or 'endoctine disruptors') that are used as the metallic foundation for nanoparticle production and are found in a variety of consumer products, such as cosmetics, household items, and processed foods, etc."
Background: ""Metalloestrogens are a class of metals shown to exert estrogenic effects through alterations of gene expression and/or modifying the activity of estrogenic receptors." These metalloestrogens "will elicit estrogenic effects and potentially change the breast anatomy. Alterations in breast anatomy correlate with increased susceptibility to the development of cancer". Note that cadmium has been shown to alter estrogenic activity in breast cancer cells (hormone positive), "leading to an increased proliferation of these tumor cells lines". But estrogen does not even have to be present to have an effect.
Which leads to the example of one metalloestrogen, cadmium...
(EDITORS' NOTE: SEE BELOW FOR THE METALLOESTROGEN, CADMIUM, FOUND IN DENTAL AMALGAMS AND BREAST BIOPSIES.
Note that cadmium is in the air - "ambient, occupation, and cigarette smoke", has a half-life of 10-30 years, and can bioaccumulate. While phosphate fertilizers and auto exhaust comprise over 50% of exposure to cadmium, cadmium may even be in the gutta percha filling in root canals.
Cadmium's Estrogenic Effects: Since estrogen does not have to be present, cadmium can even have an effect on post-menopausal women. "The actions of cadmium have provided the most compelling evidence of a correlation with breast cancer proliferation. Comparing the affinities of estrogen and cadmium for the estrogen receptor (ERa), both compounds exhibit similar affinities, yet defining cadmium action at the ERa binding ... has yet to be determined. The prevailing hypothesis is that ERa is sequestered in the inactive form - low estrogen or no estrogen. Once activated, the receptor undergoes a conformational change and enters the active state. Increasing the number of active ERa receptors will increase estrogen responsiveness. Cadmium inhibits the action of estrogen to increase the number of active ERa, suggesting that cadmium interferes with estrogen binding to the recognition site on the ERa receptor."
Conclusion: "Metalloestrogens mimic the physiologic function of estrogen and have shown an affinity for estrogen receptors. Because they can mimic estrogen, thus activating the receptor, they are considered harmful and potentially linked to breast cancer. ... Although the data are not definitive for being a causative agent, cadmium can be considered a risk factor for breast cancer development. ...In humans, a metal such as cadmium, enters the body at low concentrations but can sequester in various tissues and maintain a presence for years." The researcher believes that,"This low-level, constant, chronic exposure would be a more accurate model" to study. (EDITORS' NOTE: SEE BELOW, FOR CADMIUM IN AMALGAMS IN BREAST CANCER BIOPSIES.) (See David Wallace, Nanotoxiciology and Metalloestrogen: Possible Involvement in Breast Cancer, Toxics, 2015.)
Background: ""Metalloestrogens are a class of metals shown to exert estrogenic effects through alterations of gene expression and/or modifying the activity of estrogenic receptors." These metalloestrogens "will elicit estrogenic effects and potentially change the breast anatomy. Alterations in breast anatomy correlate with increased susceptibility to the development of cancer". Note that cadmium has been shown to alter estrogenic activity in breast cancer cells (hormone positive), "leading to an increased proliferation of these tumor cells lines". But estrogen does not even have to be present to have an effect.
Which leads to the example of one metalloestrogen, cadmium...
(EDITORS' NOTE: SEE BELOW FOR THE METALLOESTROGEN, CADMIUM, FOUND IN DENTAL AMALGAMS AND BREAST BIOPSIES.
Note that cadmium is in the air - "ambient, occupation, and cigarette smoke", has a half-life of 10-30 years, and can bioaccumulate. While phosphate fertilizers and auto exhaust comprise over 50% of exposure to cadmium, cadmium may even be in the gutta percha filling in root canals.
Cadmium's Estrogenic Effects: Since estrogen does not have to be present, cadmium can even have an effect on post-menopausal women. "The actions of cadmium have provided the most compelling evidence of a correlation with breast cancer proliferation. Comparing the affinities of estrogen and cadmium for the estrogen receptor (ERa), both compounds exhibit similar affinities, yet defining cadmium action at the ERa binding ... has yet to be determined. The prevailing hypothesis is that ERa is sequestered in the inactive form - low estrogen or no estrogen. Once activated, the receptor undergoes a conformational change and enters the active state. Increasing the number of active ERa receptors will increase estrogen responsiveness. Cadmium inhibits the action of estrogen to increase the number of active ERa, suggesting that cadmium interferes with estrogen binding to the recognition site on the ERa receptor."
Conclusion: "Metalloestrogens mimic the physiologic function of estrogen and have shown an affinity for estrogen receptors. Because they can mimic estrogen, thus activating the receptor, they are considered harmful and potentially linked to breast cancer. ... Although the data are not definitive for being a causative agent, cadmium can be considered a risk factor for breast cancer development. ...In humans, a metal such as cadmium, enters the body at low concentrations but can sequester in various tissues and maintain a presence for years." The researcher believes that,"This low-level, constant, chronic exposure would be a more accurate model" to study. (EDITORS' NOTE: SEE BELOW, FOR CADMIUM IN AMALGAMS IN BREAST CANCER BIOPSIES.) (See David Wallace, Nanotoxiciology and Metalloestrogen: Possible Involvement in Breast Cancer, Toxics, 2015.)
METALS MAY HAVE ESTROGENIC EFFECT AND MANY ARE IN AMALGAMS
CADMIUM, ARSENITE, SELENITE MIMIC ESTRADIOL IN BREAST CANCER CELLS HOW ABOUT COPPER, COBALT, NICKEL, LEAD, MERCURY, TIN, CHROMIUM, VANADATE IN BREAST CANCER CELLS?
"We have shown that, similar to estradiol, metalloestrogens, (such as copper, cobalt, nickel, lead, mercury, tin, and chromium), induce the growth and expression of estrogen-regulated genes in breast cancer cells." Martin MB et al., 2003.
The Martin MB et al. Georgetown University team has previously shown that cadmium, arsenite, and selenite mimic estradiol in breast cancer cells by activating the estrogen receptor.
How about other metals? And how do they mimic estrogen?
"The present study demonstrates that the divalent metal chlorides of copper, cobalt, nickel, lead, mercury, tin, and chromium, as well as the metal anion vanadate have a significant effect on estrogen receptor expression and activity. Similar to estradiol, these metals induce the growth of breast cancer cells, decrease the steady state amounts of ER protein and mRNA, induce the two estrogen-regulated genes, progesterone receptor and pS2, and activate the estrogen receptor in transient transfection experiments."
From Georgetown University: "We have recently identified a new, potent class of environmental estrogens referred to as 'metalloestrogens.' These metals fall into two separate subclasses, metal/metalloids anions that include arsenite, selenite, and vanadate and bivalent cations that include cadmium, cobalt, copper, nickel, chromium, lead, mercury, and tin. We have shown that, similar to estradiol, metalloestrogens induce the growth and expression of estrogen-regulated genes in breast cancer cells and in transient transfection experiments. More importantly, we have shown that cadmium, at a dose similar to the World Health Organization recommended Provisional Tolerable Daily Intake, mimic the effects of estrogen in vivo. The ability of metalloestrogens to mimic the functions of estradiol is due to their ability to form a high affinity complex within the hormone binding domain that activates the receptor." (For the Georgetown University information, see http://explore.georgetown.edu/people/martinmb/?action=viewresearch ... For the study, see Martin MB et al.,Estrogen-Like Activity of Metals in Mcf-7 Breast Cancer Cells, Endocrinology, 2003.)
How about other metals? And how do they mimic estrogen?
"The present study demonstrates that the divalent metal chlorides of copper, cobalt, nickel, lead, mercury, tin, and chromium, as well as the metal anion vanadate have a significant effect on estrogen receptor expression and activity. Similar to estradiol, these metals induce the growth of breast cancer cells, decrease the steady state amounts of ER protein and mRNA, induce the two estrogen-regulated genes, progesterone receptor and pS2, and activate the estrogen receptor in transient transfection experiments."
From Georgetown University: "We have recently identified a new, potent class of environmental estrogens referred to as 'metalloestrogens.' These metals fall into two separate subclasses, metal/metalloids anions that include arsenite, selenite, and vanadate and bivalent cations that include cadmium, cobalt, copper, nickel, chromium, lead, mercury, and tin. We have shown that, similar to estradiol, metalloestrogens induce the growth and expression of estrogen-regulated genes in breast cancer cells and in transient transfection experiments. More importantly, we have shown that cadmium, at a dose similar to the World Health Organization recommended Provisional Tolerable Daily Intake, mimic the effects of estrogen in vivo. The ability of metalloestrogens to mimic the functions of estradiol is due to their ability to form a high affinity complex within the hormone binding domain that activates the receptor." (For the Georgetown University information, see http://explore.georgetown.edu/people/martinmb/?action=viewresearch ... For the study, see Martin MB et al.,Estrogen-Like Activity of Metals in Mcf-7 Breast Cancer Cells, Endocrinology, 2003.)

* METALS IN BREAST TUMORS AND BENIGN TUMORS *
"The data suggest that pathological accumulation of transition metals in breast tissue may be closely related to the malignant growth process." Ionescu JG et al., 2006
"The autoxidation of vitamin C and phenolic compounds in the presence of heavy metals strongly increase superoxide and H2O2 generation at the tumor site, resulting in a fast depletion of the malignant cell reducing equivalents with oxidosis shift and apoptosis induction." Ionescu JG et al., 2007
"The autoxidation of vitamin C and phenolic compounds in the presence of heavy metals strongly increase superoxide and H2O2 generation at the tumor site, resulting in a fast depletion of the malignant cell reducing equivalents with oxidosis shift and apoptosis induction." Ionescu JG et al., 2007
MEDIAN LEVELS OF METALS IN 20 MALIGNANT BREAST TUMORS AND 8 BENIGN BREAST TUMORS
EXPRESSED AS ug/kg
IRON NICKEL CHROMIUM ZINC MERCURY CADMIUM
MALIGNANT 53,174 955 816 17,075 6.9 42
BENIGN 10,937 21 29 3,741 2.1 16
* NONE HAD OCCUPATIONAL EXPOSURE TO METALS
* 1/2 WERE SMOKERS
* THEY DID HAVE "DENTAL RESTORATIONS, AMALGAMS, GOLD BRIDGES OR RETAINERS".
In the Ionescu JG et al. 2006 study, the researchers explored the accumulation of heavy metals in breast cancer biopsies.
The researchers noted that, 'High levels of transition metals such as iron, nickel, chromium, copper, and lead are closely related to free radical generation, lipid peroxidation, formation of DNA strand breaks, and tumor growth in cellular systems."
Are these heavy metals present in the biopsies of breast cancer tissue as opposed to healthy tissue?
In 20 breast cancer biopsies, "A highly significant accumulation of iron, nickel, chromium, zinc, cadmium, mercury, and lead was found in the cancer samples when compared to the control group. Copper and silver showed no significant differences to the control group, whereas tin, gold, and palladium were not detectable in any biopsies."
Conclusion: "The data suggest that pathological accumulation of transition metals in breast tissue may be closely related to the malignant growth process." (See Ionescue JG et al., Increased Levels of Transition Metals in Breast Cancer Tissue, Neuor Endocrinol Lett, 2006.)
* SECOND STUDY - HOW TO HELP COUNTERACT METALS - ADD PROOXIDANT VITAMIN C OR SUBSTITUTED PHENOLS *
In 2007, the Ionescu team further concluded that these accumulated metals in breast cancer biopsies may be related to malignant growth, and "explain the anti-tumoral effects of current therapies with high doses of vitamin C or substituted phenols, respectively."
Dr. Ionescu commented on considering a new therapy with prooxidant vitamin C or phenolic compounds. "We therefore suggest that future utilization of high dose vitamin C with prooxidant character and / or combinations of substituted phenolic compounds devoid of side-effects should be seriously considered in the treatment of different malignancies. Both vitamin C and the phenolic compounds are taking advantage of the diminished capability of tumor cells to handle free radicals. Whereas free radicals are quickly scavenged in normoxic (healthy) tissues, hypoxic tumor cells are expressing low levels of ROS protective enzymes, such as superoxide dismutase, catalase, and GSH-peroxidase. Therefore, the tumor cells are much more vulnerable to free radical attack than normal cells. .... The autoxidation of vitamin C and phenolic compounds in the presence of heavy metals strongly increase superoxide and H2O2 generation at the tumor site, resulting in a fast depletion of the malignant cell reducing equivalents with oxidosis shift and apoptosis induction."
(See Ionescue JG et al., Breast Tumors Strongly Accumulate Transition Metals, Maedica - A Journal of Clinical Medicine, 2007.)
EXPRESSED AS ug/kg
IRON NICKEL CHROMIUM ZINC MERCURY CADMIUM
MALIGNANT 53,174 955 816 17,075 6.9 42
BENIGN 10,937 21 29 3,741 2.1 16
* NONE HAD OCCUPATIONAL EXPOSURE TO METALS
* 1/2 WERE SMOKERS
* THEY DID HAVE "DENTAL RESTORATIONS, AMALGAMS, GOLD BRIDGES OR RETAINERS".
In the Ionescu JG et al. 2006 study, the researchers explored the accumulation of heavy metals in breast cancer biopsies.
The researchers noted that, 'High levels of transition metals such as iron, nickel, chromium, copper, and lead are closely related to free radical generation, lipid peroxidation, formation of DNA strand breaks, and tumor growth in cellular systems."
Are these heavy metals present in the biopsies of breast cancer tissue as opposed to healthy tissue?
In 20 breast cancer biopsies, "A highly significant accumulation of iron, nickel, chromium, zinc, cadmium, mercury, and lead was found in the cancer samples when compared to the control group. Copper and silver showed no significant differences to the control group, whereas tin, gold, and palladium were not detectable in any biopsies."
Conclusion: "The data suggest that pathological accumulation of transition metals in breast tissue may be closely related to the malignant growth process." (See Ionescue JG et al., Increased Levels of Transition Metals in Breast Cancer Tissue, Neuor Endocrinol Lett, 2006.)
* SECOND STUDY - HOW TO HELP COUNTERACT METALS - ADD PROOXIDANT VITAMIN C OR SUBSTITUTED PHENOLS *
In 2007, the Ionescu team further concluded that these accumulated metals in breast cancer biopsies may be related to malignant growth, and "explain the anti-tumoral effects of current therapies with high doses of vitamin C or substituted phenols, respectively."
Dr. Ionescu commented on considering a new therapy with prooxidant vitamin C or phenolic compounds. "We therefore suggest that future utilization of high dose vitamin C with prooxidant character and / or combinations of substituted phenolic compounds devoid of side-effects should be seriously considered in the treatment of different malignancies. Both vitamin C and the phenolic compounds are taking advantage of the diminished capability of tumor cells to handle free radicals. Whereas free radicals are quickly scavenged in normoxic (healthy) tissues, hypoxic tumor cells are expressing low levels of ROS protective enzymes, such as superoxide dismutase, catalase, and GSH-peroxidase. Therefore, the tumor cells are much more vulnerable to free radical attack than normal cells. .... The autoxidation of vitamin C and phenolic compounds in the presence of heavy metals strongly increase superoxide and H2O2 generation at the tumor site, resulting in a fast depletion of the malignant cell reducing equivalents with oxidosis shift and apoptosis induction."
(See Ionescue JG et al., Breast Tumors Strongly Accumulate Transition Metals, Maedica - A Journal of Clinical Medicine, 2007.)
ROOT CANALS - DEAD TEETH
"I went to an oncologist's office and we found 70% (of cancer patients)
had a root canal on the meridian of the primary tumor, and 30% had an infection in a crown on the meridian of the primary tumor." Jerry Tennant, MD, 2015.
had a root canal on the meridian of the primary tumor, and 30% had an infection in a crown on the meridian of the primary tumor." Jerry Tennant, MD, 2015.
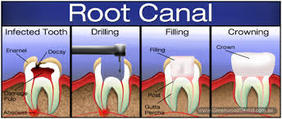
"During a root canal, the infected or inflamed pulp is removed, cleaned out, and a material, such as gutta percha, is inserted, and a crown or a filling encapsulates it.
Robert Kulacz, DDS, and Thomas Levy, MD, PHD, 2014.
Robert Kulacz, DDS, and Thomas Levy, MD, PHD, 2014.
"A root canal is a dead tooth." Jerry Tennant
Jerry Tennant MD, wrote, "A root canal is a dead tooth. If your tooth begins to hurt, your dentist may suggest that you have a root canal. This is accomplished by drilling a hole on the top of your tooth, inserting an auger, and ripping out the artery and nerve. Without a blood supply, the tooth dies. If I told you that because your appendix hurts, I am going to go into your spine and cut the nerve to the appendix so you won't fee that it hurts and then rip the artery of the appendix so it will die, I doubt you would let me do it. Dentists are the only physicians that purposely leave dead tissue in the body. They mistakenly believe that they can sterilize dead tissue and it will stay that way. It simply can not be done. If you have a piece of dead bone in your leg, and I magically sterilize it, ii will still get infected. If your big toe gets infected, and I don't remove it, you will get gangrene and die. If your appendix dies and you don't remove it, you will die from peritonitis. ALL DEAD TISSUE GETS INFECTED." (See http://tennantinstitute.us/conditions/root-canals.html.)
"A root canal is a dead tooth." Jerry Tennant
Jerry Tennant MD, wrote, "A root canal is a dead tooth. If your tooth begins to hurt, your dentist may suggest that you have a root canal. This is accomplished by drilling a hole on the top of your tooth, inserting an auger, and ripping out the artery and nerve. Without a blood supply, the tooth dies. If I told you that because your appendix hurts, I am going to go into your spine and cut the nerve to the appendix so you won't fee that it hurts and then rip the artery of the appendix so it will die, I doubt you would let me do it. Dentists are the only physicians that purposely leave dead tissue in the body. They mistakenly believe that they can sterilize dead tissue and it will stay that way. It simply can not be done. If you have a piece of dead bone in your leg, and I magically sterilize it, ii will still get infected. If your big toe gets infected, and I don't remove it, you will get gangrene and die. If your appendix dies and you don't remove it, you will die from peritonitis. ALL DEAD TISSUE GETS INFECTED." (See http://tennantinstitute.us/conditions/root-canals.html.)
ROOT CANALS
WHY CAN ROOT CANALS STILL GET INFECTED? ROLE OF IMMUNE SYSTEM.
In The Toxic Tooth, by Robert Kulacz, DDS, and Tom Levy, MD, JD, the authors discussed why bacteria can't be banished in root canals. "The American Association of Endodontists states that the presence of bacteria does not constitute infection. This is misleading since without a blood supply inside the tooth, a root canal-treated tooth, can not mount an inflammatory response. The lack of an inflammatory response actually allows the bacteria to thrive without the threat of an immune response. Further, although our bodies contain millions of bacteria that do not cause us illness, just like with real estate, it is location, location, location! It is the presence of pathogenic bacteria within tissues that should be normally free of bacteria that causes the problem How then does the American Association of Endodontists claim that the residual bacteria that caused the need for a root canal in the first place not constitute an infection?" (See Robert Kulacz, DDS and Thomas Levy, MD, JD, The Toxic Tooth, MedFox Publishing, 2014.)
ROOT CANALS
WESTON PRICE, DDS, EXPERIMENTS
HUMAN EXTRACTED ROOT CANALS IMPLANTED IN RABBIT "TYPICALLY DEVELOPED THE SAME DISEASES THAT PLAGUED THE HUMAN FROM WHOM THE TEETH HAD BEEN EXTRACTED".
In The Toxic Tooth, the authors described how Weston Price, DDS, discovered that root canals harbor bacteria, and "clearly demonstrated that both bacteria and their associated toxins readily escape from a root canal-treated tooth. In several of his experiments, he surgically implanted extracted root canal-treated teeth under the skin of rabbits These teeth were always highly toxic. He found that if the rabbits did not quickly die from the overwhelming toxicity of the implanted teeth, they typically developed the same diseases that plagued the human from whom the teeth had been extracted." (See Robert Kulacz, DDS and Thomas Levy, MD, JD, The Toxic Tooth, MedFox Publishing, 2014.)
"In one of his studies, Dr. Weston Price transferred diseases harbored by humans into rabbits, by implanting fragments of teeth from root-canals. He found that root canal fragments transplanted from a person, who had suffered a heart attack, when implanted into a rabbit, could cause a heart attack in the rabbit within only a few short weeks. The heart attack study was conducted with 100% effectiveness, while other diseases were more than 80% transferable by following this same method."
www.milesofsmilesdental.net/1409/root-canals-can-lead-to-serious-disease-including-cancer/.
www.milesofsmilesdental.net/1409/root-canals-can-lead-to-serious-disease-including-cancer/.
"My dental assistant once described an extracted root canal-treated tooth as smelling like a dead mouse that had been decomposing for a while." Robert Kulacz and Thomas Levy, MD, JD, 2014.
ROOT CANAL-TREATED TEETH
"HOTBEDS OF PATHOGENS AND TOXINS"
From The Toxic Tooth: "The overall number and diversity of microorganisms found in dental pulp infections and root canal-treated teeth is staggering. Over 400 different bacteria have ben identified in these teeth, with a high preponderance of anaerobic species. Among these bacteria are even included a wide array of spirochetes of the genus Treponema." These bacteria produce toxins, divided into endotoxins and exotoxins. While endotoxins have been mostly studied in root canal-treated teeth, as they are easier to find, exotoxins are also present. "Endotoxins are large molecules comprised of repeating carbohydrate chains attached to a lipid. They are found on the outer membranes of gram-negative bacteria and produce a strong immune response in animals. Generally endotoxins are only released when the bacteria die..... Exotoxins are created inside living bacteria and generally secreted, although they can also be released upon death of the bacteria. These toxins can destroy cells and disrupt cellular metabolism throughout the body. Well-known examples of exototoxins include botulinium toxins that causes botulism, diptheria toxins capable of causing myocarditis and tetanospasmin toxins that produces tetanus. Exotoxins are usually much more toxic than endotoxins and can readily cause cell death and even the death of the host animal or patient." (See Robert Kulacz, DDS and Thomas Levy, MD, JD, The Toxic Tooth, MedFox Publishing, 2014.)
"Root canals pose problems, as these treated teeth have a propensity to 'perpetually spew' bacteria."
Robert Kulacz, DDS and Thomas Levy, MD,JD, 2014.
ROOT CANALS
IMAGING OF ROOT CANALS
FROM 2D X-RAYS FINDING 70% OF THE ROOT CANAL INFECTIONS, TO 3D X-RAYS FINDING 91% OF THE INFECTIONS
From The Toxic Tooth: "Additional evidence of infection in root canal-treated teeth is now being revealed by recent developments in 3D cone beam computed tomography x-ray imaging. ... With conventional two-dimensional dental x-rays, much of this pathology was not visible because the periapical lesions were hidden either in front of or behind the root, or often 2-3 mm away from the radiographic apex of the tooth, thus rendering them undetectable. In one study, the 3D technique discovered infection in 21% more root canal-treated teeth than was detected with 2D x-rays. While 2D x-rays detected infection in 70% of the teeth, the 3D technique discovered infection in 91% of the same 46 teeth. Evolving 3D technology serves to show that the vast majority of root canal-treated teeth have radiological evidence indicating chronic infection." (See Robert Kulacz, DDS and Thomas Levy, MD, JD, The Toxic Tooth, MedFox Publishing, 2014.)
TESTING ROOT CANAL TOXINS
PRELIMINARY TOXIN TESTING BY BOYD HALEY, PHD, AND STUART NUNNALLY, DDS
Testing root canal toxins: Kulacz and Levy wrote, "How can we objectively measure the degree of toxicity in root canal-treated teeth? We know that the root canal procedure can not remove all the bacteria with a tooth and that over time additional bacteria will enter the mouth. ... Studies have shown that bacteria do come out of the root canal-treated tooth into the surrounding periodontal tissues. But more importantly, it is the small molecular weight exotoxins like hydrogen sulfide and methyl thiol that readily migrate out of the root canal-treated tooth."
Dr. Boyd Haley's testing: "The process that Dr. Haley developed is called nucleotide photo affinity labeling. He wanted to see if toxins coming out of a root canal-treated tooth would inhibit the activity of five key human enzymes: Phosphorylase kinase, phosphorylase A, pyruvate kinase, creatine kinase, and adenylate kinase." Note here that the root-canal treated teeth were washed three times. Why? The first two washings were to wash off any external contamination, while the third washing should then represent the toxins that come from inside the tooth that may be capable of enzyme inhibition. Testing the tooth against the five enzymes revealed that, "All of the over 5000 tested root canal-treated teeth were sufficiently infected to produce toxins. .... About 25% of these teeth showed minimal toxicity (less than 5% enzyme inhibition) while others still showed profound toxicity. The primary point to be concluded is that, even with two very prolonged washings before the third washing, measurable toxicity was detected in 100% of this series of teeth. As toxins in the tooth do not naturally occur, this is clear evidence that all of the tested rootcanal-treated teeth were sufficiently infected to produce toxins." (See Robert Kulacz, DDS and Thomas Levy, MD, JD, The Toxic Tooth, MedFox Publishing, 2014.)
Dr. Boyd Haley's testing: "The process that Dr. Haley developed is called nucleotide photo affinity labeling. He wanted to see if toxins coming out of a root canal-treated tooth would inhibit the activity of five key human enzymes: Phosphorylase kinase, phosphorylase A, pyruvate kinase, creatine kinase, and adenylate kinase." Note here that the root-canal treated teeth were washed three times. Why? The first two washings were to wash off any external contamination, while the third washing should then represent the toxins that come from inside the tooth that may be capable of enzyme inhibition. Testing the tooth against the five enzymes revealed that, "All of the over 5000 tested root canal-treated teeth were sufficiently infected to produce toxins. .... About 25% of these teeth showed minimal toxicity (less than 5% enzyme inhibition) while others still showed profound toxicity. The primary point to be concluded is that, even with two very prolonged washings before the third washing, measurable toxicity was detected in 100% of this series of teeth. As toxins in the tooth do not naturally occur, this is clear evidence that all of the tested rootcanal-treated teeth were sufficiently infected to produce toxins." (See Robert Kulacz, DDS and Thomas Levy, MD, JD, The Toxic Tooth, MedFox Publishing, 2014.)
As Robert Kulacz, DDS,and Tom Levy, MD,JD, point out, all root canal-treated teeth are and will remain infected:
"Even a tiny population of bacteria or fungi that survives in a missed canal or somewhere in the miles of dentinal tubules can multiple into a large colony." And this bacteria is insulated - "disconnected" from the immune system's surveillance, so the bacteria can thrive. "Thus, removing the pain-sensing nerves from a tooth and blocking all access to the infection-fighting system does not 'cure' the tooth."
ROOT CANALS
DO ASYMPTOMATIC ROOT CANALS' BACTERIA INHIBIT ENZYMES RELATED TO ATP PRODUCTION?
"These preliminary results suggest that root canal treated teeth inhibit the action of critically important enzymes that generate cellular ATP." Stuart Nunnally, DDS, 2012
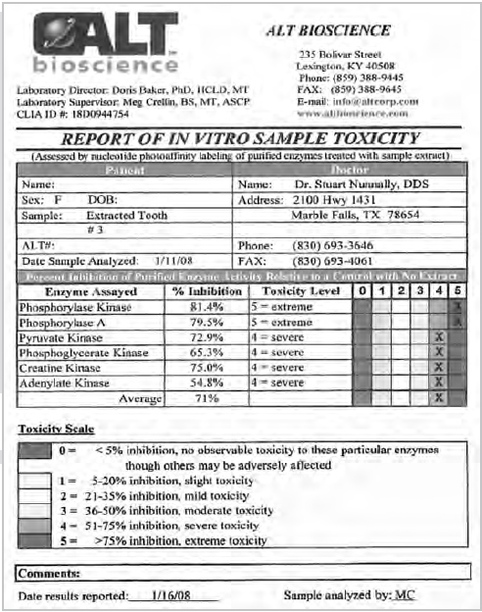
The results of enzymatic inhibition of one root canal treated tooth.
Yes ..... In a preliminary 2012 study by Stuart Nunnally, DDS.
Against a background of perceived toxicity from root canal treated teeth, Stuart Nunnally, DDS., sought to determine if asymptomatic root canals as confirmed on x-rays, would harbor ATP enzyme-inhibiting bacteria.
To this end, this researcher had 25 seemingly healthy root canal teeth that had been extracted from his patients' mouths due to concerns about their health, tested.
The extracted teeth were placed in sterile bottles. "The individual root fragments were carefully selected to minimize the impact of contamination or leaching from the restorativ materials. ... Toxicity testing was performed on all root fragments after washing them three times in distilled water, and after filtration, 10 microliters of each thrid wash sample was incubated with six enzymes (i.e., phosphorylase kinase, phosphortyase A, pyruvate kinase, phosphoglycerate kinase, creatine kinase, and adenylate kinase) to determine the degree of enzymatic inhbition."
Results: The percent of enzymatic inhibition ranged from 28% to 89%, with a median of 68%.
Conclusion and Limitations: "These preliminary results suggest that root canal treated teeth inhibit the action of critically important enzymes that generate cellular ATP." Limitations: "Since no control group was chosen, "It is impossible to know if root fragments from properly matched non-root canal treated teeth would produce less enzymatic inhibition compared to root fragments derived from root canal treated teeth. it is also difficult to correlate these in vitro findings to a patient's clinical health status. It is also possible that the root fragments were contaminated by mercury or other substances even though samples were carefully chosen to minimize these effects. None of the root fragments were analyzed or cultured. These results, therefore, can only be considered very preliminary in nature." (See Stuart Nunnally, DDS, In Vitro Enzymatic Inhibition Associated with Asymptomatic Root Canal-Treated Teeth, Journal of Orthomolecular Medicine, 2012.)
ROOT CANALS
DENTAL PATHOGENS "EMBED IN VARIOUS BODILY TISSUES"
From The Toxic Tooth: "DNA evidence shows that these dental pathogens..in root canal-treated teeth ... commonly travel to and embed in various bodily tissues." So, ...These bacteria almost never remain sequestered inside the root canal-treated tooth. ... These dental pathogens, present both in root canal-treated teeth as well as in the infections around such teeth, commonly travel to and embed in various bodily tissues." Does the bacteria go to the breast? Do breast cancer patients commonly have root canals and other infected teeth? (See Robert Kulacz, DDS and Thomas Levy, MD, JD, The Toxic Tooth, MedFox Publishing, 2014.)
ROOT CANALS AND BREAST CANCER
SO, ARE ROOT CANALS AND DISEASED TEETH ON THE BREAST MERIDIAN?
Definition: The Meridian Tooth Chart is based on acupuncture meridians, pathways of energy that span across interrelated body parts, glands and tissue. Each tooth is associated with a particular meridian, through which energy flows." (See http://iaomt.org/find-a-doctor/tooth-meridian-chart/.)
* Joseph Mercola, DO, wrote in 2014, "Infected or diseased teeth, as well as dental implants, block electrical conductivity on meridians and so can alter the health of other organs located on the same meridian and vice versa." (See http://articles.mercola.com/sites/articles/archive/2014/05/03/root-canal-alternative.aspx.)
* Joseph Mercola, DO, wrote in 2014, "Infected or diseased teeth, as well as dental implants, block electrical conductivity on meridians and so can alter the health of other organs located on the same meridian and vice versa." (See http://articles.mercola.com/sites/articles/archive/2014/05/03/root-canal-alternative.aspx.)

BREAST MERIDIAN AND TEETH
BREAST MERIDIAN CONNECTED TO TEETH #2, #3, #14, #15,# 20,# 21,# 28, #29.
CONNECTION TO THE 4th AND 5th TOOTH FROM CENTER TOOTH, RIGHT AND LEFT, UPPER AND LOWER JAW.
Veronique Desaulniers, DC, wrote, "The root canal affects your body in two ways. 1. It creates a toxic drip of bacteria that suppresses your immune system. ... "One of the toxic anaerobic bacteria that is often present in a root canal is called E. Faecalis. This particular bacterium is responsible for the formation of abscesses, pus and destruction of tissue. In fact, root canal procedures themselves release toxic bacteria and fungi into the blood. ... 2. Energetically, the toxic tooth affects the organ connected to the tooth through the acupuncture meridian system." (See http://breastcancerconqueror.com/is-your-root-canal-increasing-your-risk-for-breast-cancer/.)
BREAST MERIDIAN CONNECTED TO TEETH #2, #3, #14, #15,# 20,# 21,# 28, #29.
CONNECTION TO THE 4th AND 5th TOOTH FROM CENTER TOOTH, RIGHT AND LEFT, UPPER AND LOWER JAW.
Veronique Desaulniers, DC, wrote, "The root canal affects your body in two ways. 1. It creates a toxic drip of bacteria that suppresses your immune system. ... "One of the toxic anaerobic bacteria that is often present in a root canal is called E. Faecalis. This particular bacterium is responsible for the formation of abscesses, pus and destruction of tissue. In fact, root canal procedures themselves release toxic bacteria and fungi into the blood. ... 2. Energetically, the toxic tooth affects the organ connected to the tooth through the acupuncture meridian system." (See http://breastcancerconqueror.com/is-your-root-canal-increasing-your-risk-for-breast-cancer/.)
"Thomas Rau, M.D. is the head of the Paracelsus Cancer Clinic in Switzerland. ... Any root canal fillings are removed before any cancer treatment is started. In 2004, Dr. Rau became curious about the prevalence of root canal-filled teeth in his clinic's breast cancer patients. He examined the records of the last 150 women who had been admitted to his clinic. He found that 147 of them (98.5%) had one or more root canal-filled teeth on the same meridian (Chinese meridian system) as the original breast cancer tumor. The other three had cavitation problems." (See http://www.cancertutor.com/advdental/.)
Burton Goldberg wrote, "Each tooth relates to an acupuncture meridian, Dr. Rau explains. This means a problem in a tooth can focus its energy imbalance elsewhere in the body, in this case his patients’ breasts."http://www.burtongoldberg.com/page79.html.) Further, Burton Goldberg wrote, "Dr. Rau has created a dental chart that maps out the precise relationship between teeth, meridians, and illnesses, including cancer. The breast, for example, lies on the stomach meridian. This means that if you have a problem (such as a root canal or jaw infection) in or around the teeth situated on this meridian, said problem can block the flow of energy along the pathway of the stomach meridian, causing degeneration and eventually cancer. Like Dr. Issels before him, Dr. Rau has also found that such dental factors can also be involved in the development of other cancer." http://www.burtongoldberg.com/page79.html.
Burton Goldberg wrote, "Each tooth relates to an acupuncture meridian, Dr. Rau explains. This means a problem in a tooth can focus its energy imbalance elsewhere in the body, in this case his patients’ breasts."http://www.burtongoldberg.com/page79.html.) Further, Burton Goldberg wrote, "Dr. Rau has created a dental chart that maps out the precise relationship between teeth, meridians, and illnesses, including cancer. The breast, for example, lies on the stomach meridian. This means that if you have a problem (such as a root canal or jaw infection) in or around the teeth situated on this meridian, said problem can block the flow of energy along the pathway of the stomach meridian, causing degeneration and eventually cancer. Like Dr. Issels before him, Dr. Rau has also found that such dental factors can also be involved in the development of other cancer." http://www.burtongoldberg.com/page79.html.
COMPOSITES
THE LATE WONDERFUL DENTIST, DR. HAL HUGGINS, REMINDED US THAT TAKING OUT AN AMALGAM AND FILLING IT WITH PLASTIC COMPOSITE MATERIAL, MAY NOT BE A "WHITE KNIGHT". INSTEAD, THE COMPOSITE FILLINGS ALSO HAVE CHEMICALS THAT CAN LEACH, AND MAY CONTAIN ALUMINIUM TO MAKE THE COMPOSITE MORE VISIBLE ON AN X-RAY.

SO, YOU DECIDE TO REPLACE YOUR TEETH METAL (AMALGAMS, GOLD, ETC.) WITH COMPOSITES? ANY HARM IN COMPOSITES? ESTROGENIC?
The American Dental Association in 2008 wrote, "There is also evidence that some dental sealants, and to a lesser extent, dental composites, may contribute to very low-level BPA exposure." (Editors' Note: BPA, bisphenol A, mimics estrogen.) (See http://healthimpactnews.com/2013/bisphenol-a-released-from-dental-sealants-and-composites/#sthash.7MxTnTNO.dpuf.) While studies may differ on the amount of BPA that is leached from composites and sealants, the IAOMT (International Academy of Oral Medicine and Toxciology) commented, ""However, the issue of possible hormonal activity of extremely small doses of BPA and other known hormone mimics, in the parts per billion range and lower, presents problems not discussed in standard toxicology. In the standard model, low dose effects are not measured, but are predicted by extrapolation from high dose experiments. Advocates of the low dose view say that extremely low exposures have another mode of activity entirely – 'endocrine disruption.' " (See http://iaomt.org/bisphenol-a-dental-composites/ .)
TOXIC?
Hal Huggins, DDS. wrote, "Composites are not always the white knight, for they contain some chemicals that leach out also. Do these chemicals sound like something you want in your mouth? Acrylate, aluminum, formaldehyde, hexane, hydroquinone, phenol, polyurethane, silane, strontium, toluene and xylene. These and more constitute composite fillings. In general it is true that they are not as toxic as mercury and copper, but there are blood tests that can tell you which composites are more compatible with your immune system. Aluminum makes the composite filling last longer. The patient may not last longer, but filling longevity is the key to success in many dental offices. Higher aluminum content gives greater resistance to the rigors of life in the oral cavity. However, the aluminum appears to leach out in quantities large enough to affect nerve impulse transmission - and even gall bladder problems. Finding out the composition of a composite, or 'white filling' is formidable at best. One of the most reliable ways is to look at a filling on the X-ray. If it nearly resembles a silver-mercury filling in appearance compared with some composites that are actually hard to see on X-rays - it is probably a high aluminum filling. Having seen patient relief of symptoms on the same day of removal many times, it is difficult for us to recommend just yanking out mercury fillings and replacing them randomly with whatever the dentist has on the shelf. Are you getting the idea that dental materials provide a serious problem?" (See https://www.hugginsappliedhealing.com/dental-dangers.php.)
"I do not, for instance, recommend that .. teeth be removed from a healthy person. But I believe if they are diseased, they cause the body's natural resistance to be lowered, thus acting as an important contributory factor to tumor development. In these cases, I insist on their removal."
Josef Issels, MD,www.issels.com/publications/FocusOnFoci.
Josef Issels, MD,www.issels.com/publications/FocusOnFoci.
SO, YOU WANT TO HAVE YOUR ROOT CANAL, FOR EXAMPLE, REMOVED? HOW ABOUT CAVITATIONS? REMOVAL OF A ROOT CANAL OR OTHER TOOTH MUST INCLUDE THE PERIODONTAL LIGAMENT. OTHERWISE,
CHEMICALS MAY SEEP OUT INTO THE BODY.
" .... A cavitation is a hole within the upper or lower jaw bone. This hole is roughly the size and shape of the root that once occupied that space in bone, because that was its origin. It is an area of incomplete healing (subsequent to the removal of a tooth). .When a woman delivers a baby, she must also deliver the afterbirth. When a tooth is delivered, there is an equivalent of the afterbirth. It is called the periodontal ligament. This is a group of fibers, half of which originate within the tooth and the other half from the bone surrounding the tooth. They blend together and form a hammock-like structure that unites tooth and bone. There is normally no bony attachment between the two. When a tooth has a root canal, or is in a dying state, bacteria within the tooth produce very strong chemicals that are highly neurotoxic and kill many critical enzymes within the body. When the tooth is removed and the ligament left in place (normal procedure) these chemicals remain within the ligament and can slowly seep into the body, potentially creating disease states.If a tooth is removed and the ligament is left in place, a cap of two to three millimeters of bone heals over the top of the socket, leaving a cesspool of these chemicals lining the hole and sealed within the bone. X-ray has a hard time identifying these areas, for one is taking a picture of a piece of air within bone.After the tooth is removed, or years later when the cavitation is being cleaned, the walls of the socket must be cut out with a dental burr. Just scraping it out (curetting is the term) pushes the toxins into the lymphatic drainage system and patients frequently become ill for several days without knowing why." https://www.hugginsappliedhealing.com/dental-dangers.php
ADDITIONAL DENTAL PROBLEMS
CAVITATIONS
Cavitations pose another problem that need to be addressed.
Cavitations are holes in the jawbone from extracted teeth that have ostensibly been healed. Typically, there may be cavitations at wisdom tooth extraction sites.
Cavitations are holes in the jawbone from extracted teeth that have ostensibly been healed. Typically, there may be cavitations at wisdom tooth extraction sites.
PERIODONTAL PROBLEMS
Periodontitis, an infection of the tooth gums, is yet another problem. The bacteria may robustly promote heart disease.But what about breast cancer?
PERIODONTAL 2015 BREAST CANCER STUDY:
The Freudenheim J et al. 2015 study found that the risk of breast cancer in postmenopausal women with periodontitis is 14% higher than those without periodontal problems, and 36% higher in women who had quit smoking within the last 20 years. Why? Likely systemic inflammation and/or the bacteria "can enter the circulatory system and affect breast tissue" http://www.aacr.org/Newsroom/Pages/News-Release-Detail.aspx?ItemID=823#.Vq4SD8t56uA
Conclusion from the study: "Periodontal disease, a common chronic inflammatory disorder was associated with increased risk of postmenopausal breast cancer, particularly among smokers who quit in the past 20 years." For the study, see. Freudenheim J et al., Periodontal Disease and Breast Cancer: Prospective Cohort Study of Postmenopausal Women, Cancer Epidemiology Biomarkers and Prevention, 2015. .....
PERIODONTAL 2015 BREAST CANCER STUDY:
The Freudenheim J et al. 2015 study found that the risk of breast cancer in postmenopausal women with periodontitis is 14% higher than those without periodontal problems, and 36% higher in women who had quit smoking within the last 20 years. Why? Likely systemic inflammation and/or the bacteria "can enter the circulatory system and affect breast tissue" http://www.aacr.org/Newsroom/Pages/News-Release-Detail.aspx?ItemID=823#.Vq4SD8t56uA
Conclusion from the study: "Periodontal disease, a common chronic inflammatory disorder was associated with increased risk of postmenopausal breast cancer, particularly among smokers who quit in the past 20 years." For the study, see. Freudenheim J et al., Periodontal Disease and Breast Cancer: Prospective Cohort Study of Postmenopausal Women, Cancer Epidemiology Biomarkers and Prevention, 2015. .....
DENTAL TIPS
SOME DENTAL TIPS
1. "Remove root canal-treated teeth.
2. Have your dentist check for any other non-viable or infected teeth and decide if enough evidence supports monitoring a suspected tooth or extracting it.
3. Surgically debride cavitations.
4. Address existing gum disease and practice."
Robert Kulacz and Thomas Levy, MD, JD.
1. "Remove root canal-treated teeth.
2. Have your dentist check for any other non-viable or infected teeth and decide if enough evidence supports monitoring a suspected tooth or extracting it.
3. Surgically debride cavitations.
4. Address existing gum disease and practice."
Robert Kulacz and Thomas Levy, MD, JD.
MORE DENTAL TIPS
ORAL HYGIENE MEASURES (EXCERPTS)
TOOTH BRUSHING: "Tooth brushing should be done at least twice daily, once in the morning, and then right before bed. An electric soft toothbrush is recommended."
FLOSSING: "Flossing is recommended to manually debride the sides of the toothe and the interproximal gingival sulcus where tooth brushing does not reach. Flossing once daily at bedtime with thin unwaxed dental floss is a good routine.
ORAL WATER IRRIGATION: Oral water irrigation, known to many as the Waterpik, is esssential for restoring and maintaining gum health." Robert Kulacz, DDS, and Thomas Levy, MD, JD., 2014.
ORAL HYGIENE MEASURES (EXCERPTS)
TOOTH BRUSHING: "Tooth brushing should be done at least twice daily, once in the morning, and then right before bed. An electric soft toothbrush is recommended."
FLOSSING: "Flossing is recommended to manually debride the sides of the toothe and the interproximal gingival sulcus where tooth brushing does not reach. Flossing once daily at bedtime with thin unwaxed dental floss is a good routine.
ORAL WATER IRRIGATION: Oral water irrigation, known to many as the Waterpik, is esssential for restoring and maintaining gum health." Robert Kulacz, DDS, and Thomas Levy, MD, JD., 2014.
OIL PULLING

In the Tomar P et al. 2014 review article, the researchers stated, "The concept of oil pulling really isn't new, but it is a modified version of oil gargling... Oil pulling has been used extensively as a traditional Indian folk remedy for years to prevent decay, bleeding gums, oral malodor, dryness of throat, cracked lips, and for strengthening teeth, gums, and jaws."
"It's really amazing what oil pulling can do. It's excellent as a preventative and it can even help treat some conditions.. Now, the first thing that people experience when they start oil pulling is the improvement they see in their oral health. Things like how their teeth become whiter. Bleeding gums stop bleeding. The gums around the teeth that may be loose may tighten up around the teeth. The color of the gums would improve because it removes inflammation. Bad bread, it gets rid of bad breath, which is primarily caused by bacteria in the mouth. It helps clean off coatings on the tongue, and can even help get rid of tartar and things like that. In fact, even in infections that can be in the mouth, it will draw the infection out, so even in the abscessed tooth, now there's different degrees of severity, and so if a tooth is too far gone, there's not much you can do with it, but even some deep-seated infections can be reversed with daily oil pulling." Bruce Fife, ND., 2014.
WHY COCONUT OIL, SESAME OIL, AND OZONATED SUNFLOWER OIL MAY BE GOOD TO USE IN OIL PULLING

Coconut Oil: "Coconut oil is commonly used for oil pulling."What make coconut oil different from most other dietary oils are the basic building blocks, or fatty acids, making up the oil. The predominant composition of coconut oil is a medium chain fatty acid, whereas the majority of common edible fats in our diet are composed almost entirely of long chain fatty acids. This influences the physical and chemical properties of the oil. Coconut oil contains 92% saturated acids, approximately 50% of which is lauric acid. Recently, results from many studies revealed that the monolaurin, the monoglycerides of lauric acid from coconut oil had antimicrobial activity against various Gram-positive and Gram-negative organisms, including Escherichia vulneris, Enterobacter spp., Helicobacter pylori, Staphylococcus aureus, Candida spp., including Candida albicans, Candida glabrata, Candida tropicali, Candida parapsilosis, Candida stellatoidea, and Candida krusei, as well as enveloped viruses through the exact antibacterial mechanism of the action of coconut oil is still unclear, it was hypothesized that monolaurin and other medium-chain monoglycerides had the capacity to alter bacterial cell wall, penetrate and disrupt cell membranes, inhibit enzymes involved in energy production and nutrient transfer, leading to the death of the bacteria"
Sesame Oil: "Sesame oil is a very old cultivated crop and thought to have originated in Africa. Chlorosesamone obtained from roots of sesame has antifungal activity. Sesame lignans have antioxidant and health promoting activities. high amounts of both sesamin and sesamolin have been identified in sesame. Both sesamin and sesamolin were reported to increase both the hepatic mitochondrial and the peroxisomal fatty acid oxidation rate. Sesame seed consumption appears to increase plasma gamma tocopherol and enhanced vitamin E activity which is believed to prevent cancer and heart disease. Sesame oil is found to be effective in reducing bacterial growth and adhesion. Toxins and bacteria from the body might be expelled through the tongue and trapped in the oil and removed from the body. Sesame oil was demonstrated to have antibacterial activity against Streptococcus mutans. It contains high amounts of unsaturated fatty acids. Linolenic acid and other oleic acid are the predominant compositions. Oil pulling therapy with sesame oil significantly reduced S mutans counts in plaque and saliva of adolescents within 1 week."
Ozonated sunflower oil: "Ozonized sunflower oil showed antimicrobial activity against S. aureus, Escherichia coli. Pseudomonas aeruginosa, Enterococcus faccalis, mycobacterium spp., streptococcus pyogenes, and C. albicans. However, the activity might be due to the powerful oxidant properties of the ozone itself. Considering the antimicrobial effect of other oils, including corn oil, palm oil, rice bran oil, and soybean oil, it was proposed that small amounts of saturated fatty acid, i.e., lauric acid, in these oils may play a role in their antimicrobial properties." (See Tomar P et al., Oil Pulling and Oral Health: A Review, USS Case Reports Reviews, 2014.)
Sesame Oil: "Sesame oil is a very old cultivated crop and thought to have originated in Africa. Chlorosesamone obtained from roots of sesame has antifungal activity. Sesame lignans have antioxidant and health promoting activities. high amounts of both sesamin and sesamolin have been identified in sesame. Both sesamin and sesamolin were reported to increase both the hepatic mitochondrial and the peroxisomal fatty acid oxidation rate. Sesame seed consumption appears to increase plasma gamma tocopherol and enhanced vitamin E activity which is believed to prevent cancer and heart disease. Sesame oil is found to be effective in reducing bacterial growth and adhesion. Toxins and bacteria from the body might be expelled through the tongue and trapped in the oil and removed from the body. Sesame oil was demonstrated to have antibacterial activity against Streptococcus mutans. It contains high amounts of unsaturated fatty acids. Linolenic acid and other oleic acid are the predominant compositions. Oil pulling therapy with sesame oil significantly reduced S mutans counts in plaque and saliva of adolescents within 1 week."
Ozonated sunflower oil: "Ozonized sunflower oil showed antimicrobial activity against S. aureus, Escherichia coli. Pseudomonas aeruginosa, Enterococcus faccalis, mycobacterium spp., streptococcus pyogenes, and C. albicans. However, the activity might be due to the powerful oxidant properties of the ozone itself. Considering the antimicrobial effect of other oils, including corn oil, palm oil, rice bran oil, and soybean oil, it was proposed that small amounts of saturated fatty acid, i.e., lauric acid, in these oils may play a role in their antimicrobial properties." (See Tomar P et al., Oil Pulling and Oral Health: A Review, USS Case Reports Reviews, 2014.)

SO, HOW DO YOU DO OIL PULLING? - ONE VERSION OF OIL PULLING - DR. JOSH AXE'S STEP-BY-STEP COCONUT OIL PULLING INSTRUCTIONS
"1. Make sure to oil pull first thing in the morning right after you get out of bed, before you brush your teeth or drink anything.
2. Gently swish 1 - 2 tablespoons of coconut oil in your mouth and between your teeth for 10-20 minutes, making sure that you don't swallow any of the oil. (Do this gently so you don't wear out your jaw and cheeks!)
3. Spit the oil in the trash (not the sink so it doesn't clog up the plumbing... ask me how I know), and immediately rinse your mouth out with warm water (use salt water for added antimicrobial properties).
4. Finally, brush your teeth as normal.
5. Volila, easy as that!
I recommend oil pulling 3-4 times per week with coconut oil and also adding essential oils to your mixture." (See Dr. Josh Axe, http://draxe.com/oil-pulling-coconut-oil/.)
"1. Make sure to oil pull first thing in the morning right after you get out of bed, before you brush your teeth or drink anything.
2. Gently swish 1 - 2 tablespoons of coconut oil in your mouth and between your teeth for 10-20 minutes, making sure that you don't swallow any of the oil. (Do this gently so you don't wear out your jaw and cheeks!)
3. Spit the oil in the trash (not the sink so it doesn't clog up the plumbing... ask me how I know), and immediately rinse your mouth out with warm water (use salt water for added antimicrobial properties).
4. Finally, brush your teeth as normal.
5. Volila, easy as that!
I recommend oil pulling 3-4 times per week with coconut oil and also adding essential oils to your mixture." (See Dr. Josh Axe, http://draxe.com/oil-pulling-coconut-oil/.)
SO, HOW DO YOU DO OIL PULLING?
WHAT IF YOU HAVE DENTAL FILLINGS, CROWNS? WILL OIL PULLING LOOSEN THEM?
Dr. Coconut (Bruce Fife, ND) wrote, "Occasionally, people report that they have lost fillings or crowns when they started oil pulling. Others are hesitant to try oil pulling in fear that it might loosen their dental work.
Let me ease your fears. Oil pulling will not and can not loosen properly placed crowns or fillings. The only time oil pulling will affect crowns or fillings is if the teeth underneath have decayed and are full of infection. In this case, the foundation on which the crowns or fillings are secured to is badly decayed and unable to hold the dental material. Oil pulling removes bacteria, pus, and mucus. It can not pull out porcelain, amalgam, or composite dental materials from the mouth. If you have fillings or crowns, you are completely safe.
If, however, a filling or crown does come loose, be thankful. This indicates that the underlying tooth is rotting and full of infection. This infection is spreading throughout your mouth and your entire body. You need to have it removed as soon as possible. If oil pulling brought your attention to this problem, you are lucky, because now you know the problem exists and you can take care of it without experiencing further harm."
(See Bruce Fife, ND, http://www.coconutresearchcenter.org/hwnl_8-1.htm.)
WHY DOES OIL PULLING WORK?
Interviewer Jack Miller, CTN, asked Bruce Fife, ND, about why oil pulling works.
"...One of the reasons why oil pulling works so well, and why it works better than antiseptic mouthwashes is because it's a fat, and fats attract, and fat and water repel. Any time you do any cooking, you experience how oil floats on top of water and all that. Well, in your mouth, the oil attracts the bacteria, or the bacteria actually attracts to the oil because the membrane surrounding the bacteria is made of fat, fatty acid, and so it just automatically absorbs into the oil, so when you're swishing it around and you're pushing it through your teeth and around your gums, it's kind of like a vacuum cleaner that's just sucking up all this bacteria, as well as the mucus and plaque and other things like that. And when you spit it out, your mouth is going to be much cleaner."
Interviewer Jack Miller then asked if oil pulling helps to give the good flora a chance to repopulate.
"Basically, what oil pulling is, is putting some oil in your mouth and swishing it around, as as you do that, the oil attracts and pulls out bacteria, viruses, fungi, mucus, plaque, toxins, and then when you spit it out, you're removing those toxins, those bacteria and such from your mouth, making your mouth cleaner and healthier. Now lots of people tend to think that their mouth is separated from the body, but what goes on in your mouth really, you know, affects the entire body. And so the bacteria in your mouth not only can cause cavities and gum disease, but bacteria can seep into the blood stream and circulate through the body, and it often affects different parts of the body. The bacteria can go to your heart, or to your liver, or into your kidneys, or to your joints, or to your brain. And when it goes to these areas of the body, it can cause different types of health problems such as going to your joints, it can lead to arthritis. If the bacteria goes to your brain, it can lead to dementia, if it goes to you heart, it could lead to heart failure. And so, bacteria in your mouth can actually promote a wide variety of disease or health problems throughout the body. And, for the example, the bacteria in your mouth can go to the heart. In fact, when you go to the dentist, and if you've had any heart condition, the dentist will prescribe antibiotics for you because he knows that as he works on your mouth, he's going to release more bacteria into your system, and that bacteria can go to the heart and cause heart failure. Also, the bacteria can go to your brain and cause dementia, and it's interesting the reason on this is that they will take bacteria from people who have died from dementia, and analyze it, they'll do DNA testing, and they will find that it's the exact same bacteria that is in the patient's mouth, so they know for sure where the bacteria came from. You know, more studies are being done. A couple of more studies regarding oil pulling have been done. One that I actually mentioned where a professor of dentistry in Canada who tried oil pulling as a means to treat the Sjogren's disease which is a disease which causes a dryness, a dry eyes and dry mouth, and she found that it helps stimulate the flow of fluids to help with that condition, and in her study, she also found that it was very effective in reducing the bacterial count in the mouth. So this is just more evidence that oil pulling really does work in reducing the bacterial load in the mouth, and it's not just studies coming from India, but also from Canada and elsewhere."
(See http://nhsofarizona.com/oil-pulling/.)
COCONUT OIL VERSUS MOUTHWASH (CHLORHEXIDINE) IN PLAQUE AND GINGIVITIS IN ORAL HEALTH - WHICH IS BETTER?
The same!... According to the Peedikavil FC et al. 2015 study.
The chlorhexidine-containing mouthwash and coconut oil pulling have comparable results upon plaque formation and plaque-related gingivitis.
Background: Coconut oil's medium chain fatty acids, as opposed to long chain fatty acids, have an influence on coconut oil's biochemistry. "Coconut oil contains 92% saturated acids, approximately 50% of which is lauric acid. Human breast milk is the only other naturally occurring substance with such a high concentration of lauric acid. Lauric acid has proven anti-inflammatory effects and antimicrobial effects."
In the Peedikavil FC et al. study, "60 age matched adolescent boys and girls in the age-group of 16-18 years with plaque induced gingivitis were included in the study and oil pulling was included in their oral hygiene routine. The study period was 30 days. Plaque and gingival indices of the subjects were assessed at baseline days 1,7,15 and 30."
Results: "A statistically significant decrease in the plaque and gingival indices was noticed from day 7 and the scores continued to decrease during the period of study."
How does it work? "In oil pulling, as the oil is swished in the mouth, the mechanical shear forces exerted on the oil leads to its emulsification and the surface area of the oil is greatly increased. The oil film thus formed on the surface of the teeth and the gingiva can reduce plaque adhesion and bacterial co- aggregation. It was also proposed that the alkalis in the saliva can react with the oil leading to saponification and formation of a soap like substance which can reduce the adhesion of plaque. Coconut oil has a high saponification value and is one of the most commonly used oil in making soaps."
Conclusion: "In our study there was a 50% decrease in the plaque and gingival index scores in 4 weeks which is comparable to the decrease produced by chlorhexidine (an antimicrobial found in mouthwash). " Note that, while this study did not examine coconut oil's antimicrobial effects, the "monolaurin in coconut oil may help in its "significant antimicrobial activity against Escherichia vulneris, Enterobcater spp., Helicobacter pylori, Staphylococcus aureus, Candida spp., including C. albicans, C. glabrata, C. tropicalis, C. parapsilosis, C. stellatoidea and C. krusei. Studies also show that coconut oil is affective against S. mutans and C. albicans in an in vitro oral biofilm model." (See Peedikavil FC et al., Effect of Coconut Oil in Plaque Related Gingivitis - A Preliminary Report, Niger Med J, 2015.)
DENTISTRY FUTURE
FUTURE USE OF ELECTRICITY AND LASERS TO HOPEFULLY OBVIATE USING METALS IN MOUTH
*ELECTRICITY
We all naturally remineralize our teeth via minerals in saliva and food. Losing minerals - such as calcium and phosphate - can lead to decay.
The Reminova company has created a device that can hasten remineralization without using injections or drilling in tooth repair. Thus, no metals are needed! From a 2015 Reuters article, " A patient's tooth is first conditioned and cleansed to separate any decayed tissue or organic material that has built up in the lesion. Once clean, the tooth enamel is ready for the treatment. They've called this process Electrically Assisted Enhanced Remineralization (EAER). It uses a tiny electrical current of a few micro Amps that don't cause any physical sensation in the patient to introduce natural minerals back into the clean lesion. The electrical field pushes the mineral ions into the cavity, triggering remineralization from the deepest part of the lesion." Thus, calcium and phosphate will bond to the enamel. (See Reuters, http://www.reuters.com/article/2015/08/25/us-dental-device-idUSKCN0QU21C20150825, 2015.)
*LASERS
In the Arany P et al. 2014 study, the researchers studied the effects of low power laser therapy on dentin teeth repair.
Basically, these researchers were able to employ just a low power laser to trigger dental stem cells to form dentin. Importantly, dentin is the "bone-like structure under your teeth's enamel".
How does the low power laser work? The laser creates ROS, which activates transforming growth factor beta-1(TGF-B1), which then directs dental stem cells differentiation for regeneration.
"Laser-activated TGF-β1 was capable of differentiating human dental stem cells in vitro. Further, an in vivo pulp capping model in rat teeth demonstrated significant increase in dentin regeneration after low power laser therapy treatment."
Conclusion:. "The ability of low power laser therapy to activate an endogenous morphogen to direct resident stem cell differentiation—in this case, dental stem cell—adds a new, potent tool to the regenerative armamentarium. This study elucidated both the efficacy and the primary mechanistic role of low power laser therapy and ROS–TGF-β1 in mediating dentin regeneration. .... Given the broad range of roles that ROS and TGF-β can mediate in vivo and the popularity of laser devices in current clinical settings, the mechanistic insights from this study could also promote clinical translation of low power laser treatments to modulate pain, inflammation, or immune responses, and promote tissues regeneration of bone, neural, vascular, and muscle tissues."
(For the study, see Arany P, Photactivation of Endogenous Latent Transforming Growth Factor-B1 Directs Dental Stem Cell Differentiation for Regeneration, Sci Trans Med, 2014. ... For the article, see Kusek K., Noninvasive Laser Therapy Could Radically Shift Dental Treatment and lead to a Host of Broader Clinical Application in Regenerative Medicine, Wyss Institute, 2015.)
THE EDITORS CAN'T REPEAT ENOUGH:
PLEASE SEEK A COMPETENT BIOLOGICAL DENTIST TO EVALUATE YOUR DENTAL PROBLEMS AND REMEDIES.
AS DR. HAL HUGGINS COMMENTED ABOUT COMPOSITES,
"Are you getting the idea that dental materials
provide a serious problem?"
PLEASE SEEK A COMPETENT BIOLOGICAL DENTIST TO EVALUATE YOUR DENTAL PROBLEMS AND REMEDIES.
AS DR. HAL HUGGINS COMMENTED ABOUT COMPOSITES,
"Are you getting the idea that dental materials
provide a serious problem?"