BIOPSY
BIOPSY INTRO
"If you find changes or something unusual in one of your breasts, it’s important to see a health care provider as soon as possible. But keep in mind that most breast changes are not cancer. Just because your provider wants you to have a biopsy does not mean you have breast cancer. (A biopsy is when a piece of tissue is taken out and looked at under a microscope.) In fact, most biopsy results are not cancer. But the only way to know for sure is to take out and test tissue from the suspicious area of the breast. Non-cancerous breast conditions are very common, and they are never life threatening. The two main types are fibrosis and/or cysts and other non-cancerous or benign breast tumors."
http://www.cancer.org/treatment/understandingyourdiagnosis/examsandtestdescriptions/forwomenfacingabreastbiopsy/breast-biopsy-benign-breast-conditions
SKIP THE BIOPSY? HAVE THE WHOLE TUMOR REMOVED?
EDITORS' NOTE
In this SURGERY-BIOPSY section, one study suggests that a biopsy is merely a "snapshot" of a heterogeneous cancer tumor that may be "useful", but also may be misleading for the future. Around 63%-69% of the mutations are not found in every biopsy sample, and only about 1/3 of the mutations are found in every sample. Furthermore, in another study, the commonly used core needle biopsy was found to "significantly increase" distant metastases in mice that had been biopsied as opposed to non-biopsied mice.
Does the medical standard of care promote a biopsy? But why have a biopsy? Why do it in two steps - a biopsy, then surgery? Wouldn't it be prudent to just have the WHOLE TUMOR surgically taken out? Indeed, have the whole tumor excised, altogether removed?
EDITORS' NOTE
In this SURGERY-BIOPSY section, one study suggests that a biopsy is merely a "snapshot" of a heterogeneous cancer tumor that may be "useful", but also may be misleading for the future. Around 63%-69% of the mutations are not found in every biopsy sample, and only about 1/3 of the mutations are found in every sample. Furthermore, in another study, the commonly used core needle biopsy was found to "significantly increase" distant metastases in mice that had been biopsied as opposed to non-biopsied mice.
Does the medical standard of care promote a biopsy? But why have a biopsy? Why do it in two steps - a biopsy, then surgery? Wouldn't it be prudent to just have the WHOLE TUMOR surgically taken out? Indeed, have the whole tumor excised, altogether removed?

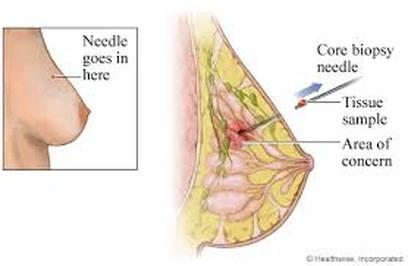
CORE NEEDLE BIOPSY - Likely, a core needle biopsy will be offered.
TYPES OF BIOPSY - EXCERPTS FROM THE AMERICAN CANCER SOCIETY
" *Core Needle Biopsy:
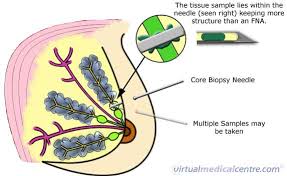
A core needle biopsy is much like a fine needle aspiration biopsy. A slightly larger, hollow needle is used to withdraw small cylinders (or cores) of tissue from the abnormal area in the breast. A core needle biopsy is most often done in the doctor’s office with local anesthesia (you are awake but your breast is numbed). The needle is put in 3 to 6 times to get the samples, or cores. This takes longer than a fine needle aspiration biopsy, but it’s more likely to give a clear result because more tissue is taken to be checked
*Fine Needle Aspiration Biopsy
In fine needle aspiration biopsy, the doctor (a pathologist, radiologist, or surgeon) uses a very thin needle attached to a syringe to withdraw (aspirate) a small amount of tissue from the suspicious area. ...A fine needle aspiration biopsy can sometimes miss cancer if the needle does not get a tissue sample from the area of cancer cells. If it doesn’t give a clear diagnosis, or your doctor still has concerns, a second biopsy or a different type of biopsy should be offered.
*Stereotactic Core Needle Biopsy:
A stereotactic core needle biopsy uses x-ray equipment and a computer to analyze pictures of the breast. The computer then pinpoints exactly where in the abnormal area the needle tip needs to go. This is often done to biopsy suspicious microcalcifications (tiny calcium deposits) when a tumor cannot be felt or seen on ultrasound.
*Vacuum-Assisted Core Biopsy :
Vacuum-assisted biopsies can be done with systems like the Mammotome® or ATEC® (Automated Tissue Excision and Collection). For these procedures, the skin is numbed and a small cut (less than ¼ inch) is made. A hollow probe is put in through the cut and guided into the abnormal area of breast tissue using x-rays, ultrasound, or MRI. A cylinder of tissue is then pulled into the probe through a hole in its side, and a rotating knife inside the probe cuts the tissue sample from the rest of the breast. These methods allow multiple tissue samples to be removed through one small opening. They are also able to remove more tissue than a standard core biopsy. Vacuum-assisted core biopsies are done in outpatient settings. No stitches are needed, and there’s usually very little scarring
*MRI-Guided Biopsy:
Sometimes the biopsy is guided by MRI. For instance, with the ATEC system discussed above, you lay face down on a special table with an opening that your breast fits into. Computers are then used to find the tumor, plot its location, and help aim the probe into the tumor. This is helpful for women with a suspicious area that can only be found by MRI."
(See http://www.cancer.org/treatment/understandingyourdiagnosis/examsandtestdescriptions/forwomenfacingabreastbiopsy/breast-biopsy-biopsy-types.)
Exploring the potential problems of finding smaller, pre-metastatic breast cancers on digital mammograms and testing with core needle biopsies.
CORE NEEDLE BIOPSIES ARE FAVORED
NOW EVEN SMALLER, PRE-METASTATIC BREAST CANCERS ARE BEING FOUND ON DIGITAL MAMMOGRAMS - WITH CORE NEEDLE BIOPSY, "POTENTIAL HARMS" UPON SPREADING TUMOR CELLS?
"CNB (core needle biopsy) and fine needle aspiration are favored over open incisional or excisional biopsies because they are less invasive, produce a smaller cosmetic post-operative footprint, and result in faster patient recovery. This is particularly appealing given that the majority of biopsied breast lesions are ultimately ruled benign. Furthermore, in addition to distinguishing invasive from non-invasive cancer, tissue obtained from CNB can be used to perform nucleic acid analysis, immunohistochemistry, or analysis of prognostic biomarkers. As a consequence, stereotactic or ultrasonographically guided CNB is currently the predominant biopsy method employed in breast cancer management ....
Our experimental findings demonstrate for the first time that in the setting of malignant breast cancer, performance of a CNB is associated with a significantly increased incidence of pulmonary metastases. We also show that an additional impact of CNB includes creation of a distinctly immunosuppressive and pro-metastatic tumor microenvironment...
In this era of digital mammography when smaller breast cancers are being detected, presumably in a pre-metastatic state, biologic knowledge of the potential harms associated with the traditional workup of breast cancer through the application of a CNB needs to be considered."
Methange E et al., 2014.
NOW EVEN SMALLER, PRE-METASTATIC BREAST CANCERS ARE BEING FOUND ON DIGITAL MAMMOGRAMS - WITH CORE NEEDLE BIOPSY, "POTENTIAL HARMS" UPON SPREADING TUMOR CELLS?
"CNB (core needle biopsy) and fine needle aspiration are favored over open incisional or excisional biopsies because they are less invasive, produce a smaller cosmetic post-operative footprint, and result in faster patient recovery. This is particularly appealing given that the majority of biopsied breast lesions are ultimately ruled benign. Furthermore, in addition to distinguishing invasive from non-invasive cancer, tissue obtained from CNB can be used to perform nucleic acid analysis, immunohistochemistry, or analysis of prognostic biomarkers. As a consequence, stereotactic or ultrasonographically guided CNB is currently the predominant biopsy method employed in breast cancer management ....
Our experimental findings demonstrate for the first time that in the setting of malignant breast cancer, performance of a CNB is associated with a significantly increased incidence of pulmonary metastases. We also show that an additional impact of CNB includes creation of a distinctly immunosuppressive and pro-metastatic tumor microenvironment...
In this era of digital mammography when smaller breast cancers are being detected, presumably in a pre-metastatic state, biologic knowledge of the potential harms associated with the traditional workup of breast cancer through the application of a CNB needs to be considered."
Methange E et al., 2014.
BREAST CANCER BIOPSIES INCREASE INFLAMMATION, ENHANCE ADJACENT CANCER CELL PROLIFERATION IN MICE - 2016 STUDY
In the Szalayova G et al. 2016 study, the researchers sought to determine if diagnostic needle biopsies for breast cancer trigger an inflammatory response, and what the consequential effect of this inflammation may be on residual tumor cells.
This study found that "diagnostic core needle biopsies trigger a selective recruitment of inflammatory cells at the site of the biopsy, and they persist for extended periods of time" Not only were there macrophages (white blood cells that engulf and digest microbes, cancer cells, etc), but eosinophils (that can act as pro-inflammatory white blood cells) were at the site of the biopsy.
BREAST CANCER BIOPSIES INCREASE INFLAMMATION, ENHANCE ADJACENT CANCER CELL PROLIFERATION IN MICE - 2016 STUDY
In the Szalayova G et al. 2016 study, the researchers sought to determine if diagnostic needle biopsies for breast cancer trigger an inflammatory response, and what the consequential effect of this inflammation may be on residual tumor cells.
This study found that "diagnostic core needle biopsies trigger a selective recruitment of inflammatory cells at the site of the biopsy, and they persist for extended periods of time" Not only were there macrophages (white blood cells that engulf and digest microbes, cancer cells, etc), but eosinophils (that can act as pro-inflammatory white blood cells) were at the site of the biopsy.
The study "importantly" showed "that biopsy causes an increase in the proliferation rate of tumor cells located in the area adjacent to the biopsy". And, "Therefore, biopsy-induced inflammation could have an impact on residual tumor cell progression and/or metastasis in human breast cancer."
Szalayova G et al., Human Breast Cancer Biopsies Induce Eosinophil Recruitment and Enhance Adjacent Cancer Cells Proliferation, Breast Can Res Treat, 2016
CORE NEEDLE BIOPSY OF BREAST CANCER TUMORS
"SIGNIFICANTLY INCREASED DISTANT METASTASES ABOVE THAT WHICH WOULD BE EXPECTED WITHOUT BIOPSY " IN MICE
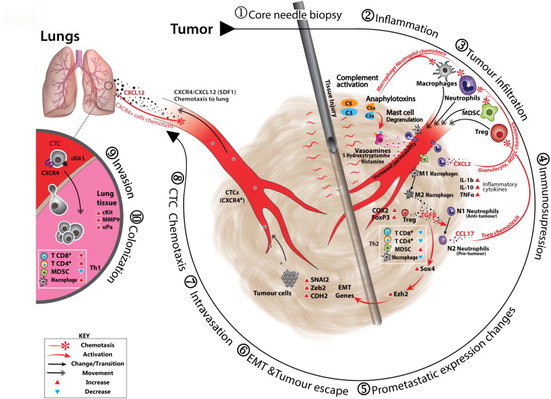
HERE IS AN ILLUSTRATION OF A CORE NEEDLE BIOPSY WITH ATTENDANT TISSUE DAMAGE CAUSING A CASCADE OF PRO-METASTATIC EXPRESSION CHANGES LEADING TO LUNG METASTASES IN MICE.
-------------------------
EXCERPTS FROM
The Mathenge E et al., 2014 study.
* In a mouse model, a core needle biopsy was associated with increased lung metastases.
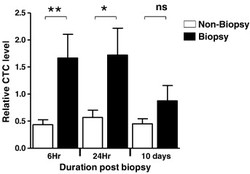
*GRAPH ABOVE: "The core needle biopsy promotes increased frequency of CTCs (circulating tumor cells) in peripheral blood Blood collected from biopsied and non- biopsied mice at 6 hours, 24 hours, and 10 days post biopsywas analyzed."
In the Mathenge E et al. 2014 study, the researchers "experimentally determined whether core needle biopsy of breast cancer tumors results in increased distant metastases and examined important resultant changes in the primary tumor and tumor microenvironment associated with this outcome".
For their study, mice were implanted with murine mammary tumor cells. After having core needle biopsies, the mice, emulating humans, had their whole tumors removed. Upon metastasis, the tumor growth, lung metastasis, CTCs, gene expressions, the microenvironment, and immunologic markers were compared to non-biopsied mice.
Results:
*"Mice with biopsied tumors developed significantly more lung metastases compared to non-biopsied mice."
*Not just more lung tumors in the biopsied mice, but an increasing immunosuppressive microenvironment! There was," ... A higher frequency of myeloid-derived suppressor cells accompanied by reduced CD4 + T cells, CD8 + T cells (that are helper T cells in the immune system) and macrophages."
*In addition, there was "up-regulation in the expression of SOX4, Ezh2, and other key epithelial-mesenchymal transition genes (epithelial cells lose their adhesion and start their migration), as well as increased circulating tumor cell levels among the biopsy group."
Conclusion: "Core needle biopsy creates an immunosuppressive tumor microenvironment, increases epithelial-mesenchymal transition, and facilitates release of circulating tumor cells, all of which contribute to the observed increase in development of distant metastases." EDITORS' NOTE: Importnatly, even ten days post-biopsy, there were more circulating tumor cells in the mice that had the biopsy than the non-biopsied mice. (See Mathenge E et al., Core Needle Biopsy of Breast Cancer Tumors Increases Distant Metastases in a Mouse Model, 2014.)
In the Mathenge E et al. 2014 study, the researchers "experimentally determined whether core needle biopsy of breast cancer tumors results in increased distant metastases and examined important resultant changes in the primary tumor and tumor microenvironment associated with this outcome".
For their study, mice were implanted with murine mammary tumor cells. After having core needle biopsies, the mice, emulating humans, had their whole tumors removed. Upon metastasis, the tumor growth, lung metastasis, CTCs, gene expressions, the microenvironment, and immunologic markers were compared to non-biopsied mice.
Results:
*"Mice with biopsied tumors developed significantly more lung metastases compared to non-biopsied mice."
*Not just more lung tumors in the biopsied mice, but an increasing immunosuppressive microenvironment! There was," ... A higher frequency of myeloid-derived suppressor cells accompanied by reduced CD4 + T cells, CD8 + T cells (that are helper T cells in the immune system) and macrophages."
*In addition, there was "up-regulation in the expression of SOX4, Ezh2, and other key epithelial-mesenchymal transition genes (epithelial cells lose their adhesion and start their migration), as well as increased circulating tumor cell levels among the biopsy group."
Conclusion: "Core needle biopsy creates an immunosuppressive tumor microenvironment, increases epithelial-mesenchymal transition, and facilitates release of circulating tumor cells, all of which contribute to the observed increase in development of distant metastases." EDITORS' NOTE: Importnatly, even ten days post-biopsy, there were more circulating tumor cells in the mice that had the biopsy than the non-biopsied mice. (See Mathenge E et al., Core Needle Biopsy of Breast Cancer Tumors Increases Distant Metastases in a Mouse Model, 2014.)
VALUE OF A BIOPSY IF INTRATUMORAL DIVERSITY? BIOPSY AREAS QUITE DIFFERENT ON A MOLECULAR LEVEL
"Just as different types of tumors have distinct genetic mutations, so do separate parts of the same tumor." Ed Yong, Nature Magazine, 2012.
SUMMARY OF GERLINGER M ET AL., 2012 STUDY
"Concept:
A single biopsy may not be representative of the entire tumor.
Major Finding:
One tumor can contain unique mutations in distinct regions.
Impact:
Intratumoral variation may confound prognostics and personalized medicine."
(See Cancer Discovery, 2012,http://cancerdiscovery.aacrjournals.org/content/2/4/300.2.full.)
"Concept:
A single biopsy may not be representative of the entire tumor.
Major Finding:
One tumor can contain unique mutations in distinct regions.
Impact:
Intratumoral variation may confound prognostics and personalized medicine."
(See Cancer Discovery, 2012,http://cancerdiscovery.aacrjournals.org/content/2/4/300.2.full.)
A biopsy is supposed to determine what kind of breast cancer a person has and how to best treat the cancer. But what if the biopsy comes from the wrong part of the tumor and misses mutations, etc? Could this lead to a missed diagnosis?
In the Gerlinger M et al. 2012 study, the researchers studied intratumor heterogeneity. "Intratumor heterogeneity may foster tumor evolution and adaptation and hinder personalized-medicine strategies that depend on results from single tumor-biopsy samples."
The researchers examined several biopsies from the same kidney cancer tumors. These were biopsy samples from both the primary tumor as well as the metastatic sites. The import of the heterogeneity? An interview with one of the researchers, plus an article about the study helped flesh out tumor diversity.
The Cancer Network interviewed one of the study's researchers, Charles Swanton, MD, PHD.
Dr. Swanton posed the threshold question: "...How many mutations are present in every biopsy, compared with those present in one biopsy or one or more biopsies but not all biopsies?"
Answer: "...We found that on the average, somewhere between 63% to 69% of mutations were not present in every biopsy sampled. So, approximately one-third of mutations were present in every region. .... What we are seeing is that the primary metastatic site evolves independently and that there are major differences between samples within the same metastatic site as well."
Although this study was on kidney cancer, "What we are seeing is evidence of heterogeneity of individual tumors across many different tumor types, including breast cancer, colorectal cancer, ovarian cancer, esophageal cancer, and other tumor types. We are seeing a diversity of somatic copy numbers (these are copies of genes) and mutational events that may be spatially separated or indeed heterogeneous within one biopsy."
How about a small tumor? "... My hunch would be that heterogeneity within an individual tumor is likely to be less profound with less bulky tumors."
Dr. Swanton observed, "So, what can we take home from this? Well, what I think we can take home from this is that a single biopsy snapshot picture of the genomic basis of the disease of one point in time may obviously be useful but may also not give the full potential picture of the cancer’s potential evolutionary path for the following years in an individual patient."
Ed Yong, in Nature Magazine in 2012, commented ......
In his wonderful article, Ed Yong wrote about why cancer may be so difficult to "study and treat". He commented, " A clinician's conclusion about prognosis or the best course of treatment can be contradictors depending on which part of the tumor the biopsy is taken from. ... For example, the first patient's tumor had split down two lines. One small part had double the usually tally of chromosomes and had seeded all the secondary tumors in the patient's chest. The other branch had spawned the rest of the primary tumor's mass."
Here is a good explanation of the problems with single biopsies. "The diversity of a tumor could explain why scientists have struggled to find clinically useful biomarkers - substances produced by the body that indicate the presence or nature of a cancer. Biomarker studies usually rely on a single biopsy, which may be misleading. In different parts of a tumor, Swanton's team found genetic signatures associated with both good and bad prognosis."
Further, "The findings could also explain why many treatments eventually stop working. Cancer drugs often target cells with specific mutations, and those might exist only in restricted parts of a tumor. Other, unaffected cells, might as as an 'evolutionary reservoir' that allows the tumor to grow again, regenerating heads of the mythical hydra. This could explain why some patients with kidney cancer fare better if surgeons remove their main tumor even if the cancer has spread. 'It may be that by removing the evolutionary reservoir of diversity, you improve a patient's outcome,' says Swanton. 'There is less material for the tumor to adapt to environmental pressures.' "
Conclusion from study:
"Genomics analyses from single tumor-biopsy specimens may underestimate the mutational burden of heterogeneous tumors. Intratumor heterogeneity may explain the difficulties encountered in the validation of oncology biomarkers owing to sampling bias, contribute to Darwinian selection of preexisting drug-resistant clones, and predict therapeutic resistance." (For the study, see Gerlinger M et al., Intratumor Heterogeneity and Branched Evolution Revealed by Multiregion Sequencing, N Engl J Med, 2012. For the Charles Swanton, MD, PHD interview, see http://www.cancernetwork.com/podcasts/understanding-complex-tumor-heterogeneity. For the Ed Yong Nature Magazine article, Biopsy Gives Only a Snapshot of Tumor Diversity, 2012, see http://www.nature.com/news/biopsy-gives-only-a-snapshot-of-tumour-diversity-1.9998.)
In the Gerlinger M et al. 2012 study, the researchers studied intratumor heterogeneity. "Intratumor heterogeneity may foster tumor evolution and adaptation and hinder personalized-medicine strategies that depend on results from single tumor-biopsy samples."
The researchers examined several biopsies from the same kidney cancer tumors. These were biopsy samples from both the primary tumor as well as the metastatic sites. The import of the heterogeneity? An interview with one of the researchers, plus an article about the study helped flesh out tumor diversity.
The Cancer Network interviewed one of the study's researchers, Charles Swanton, MD, PHD.
Dr. Swanton posed the threshold question: "...How many mutations are present in every biopsy, compared with those present in one biopsy or one or more biopsies but not all biopsies?"
Answer: "...We found that on the average, somewhere between 63% to 69% of mutations were not present in every biopsy sampled. So, approximately one-third of mutations were present in every region. .... What we are seeing is that the primary metastatic site evolves independently and that there are major differences between samples within the same metastatic site as well."
Although this study was on kidney cancer, "What we are seeing is evidence of heterogeneity of individual tumors across many different tumor types, including breast cancer, colorectal cancer, ovarian cancer, esophageal cancer, and other tumor types. We are seeing a diversity of somatic copy numbers (these are copies of genes) and mutational events that may be spatially separated or indeed heterogeneous within one biopsy."
How about a small tumor? "... My hunch would be that heterogeneity within an individual tumor is likely to be less profound with less bulky tumors."
Dr. Swanton observed, "So, what can we take home from this? Well, what I think we can take home from this is that a single biopsy snapshot picture of the genomic basis of the disease of one point in time may obviously be useful but may also not give the full potential picture of the cancer’s potential evolutionary path for the following years in an individual patient."
Ed Yong, in Nature Magazine in 2012, commented ......
In his wonderful article, Ed Yong wrote about why cancer may be so difficult to "study and treat". He commented, " A clinician's conclusion about prognosis or the best course of treatment can be contradictors depending on which part of the tumor the biopsy is taken from. ... For example, the first patient's tumor had split down two lines. One small part had double the usually tally of chromosomes and had seeded all the secondary tumors in the patient's chest. The other branch had spawned the rest of the primary tumor's mass."
Here is a good explanation of the problems with single biopsies. "The diversity of a tumor could explain why scientists have struggled to find clinically useful biomarkers - substances produced by the body that indicate the presence or nature of a cancer. Biomarker studies usually rely on a single biopsy, which may be misleading. In different parts of a tumor, Swanton's team found genetic signatures associated with both good and bad prognosis."
Further, "The findings could also explain why many treatments eventually stop working. Cancer drugs often target cells with specific mutations, and those might exist only in restricted parts of a tumor. Other, unaffected cells, might as as an 'evolutionary reservoir' that allows the tumor to grow again, regenerating heads of the mythical hydra. This could explain why some patients with kidney cancer fare better if surgeons remove their main tumor even if the cancer has spread. 'It may be that by removing the evolutionary reservoir of diversity, you improve a patient's outcome,' says Swanton. 'There is less material for the tumor to adapt to environmental pressures.' "
Conclusion from study:
"Genomics analyses from single tumor-biopsy specimens may underestimate the mutational burden of heterogeneous tumors. Intratumor heterogeneity may explain the difficulties encountered in the validation of oncology biomarkers owing to sampling bias, contribute to Darwinian selection of preexisting drug-resistant clones, and predict therapeutic resistance." (For the study, see Gerlinger M et al., Intratumor Heterogeneity and Branched Evolution Revealed by Multiregion Sequencing, N Engl J Med, 2012. For the Charles Swanton, MD, PHD interview, see http://www.cancernetwork.com/podcasts/understanding-complex-tumor-heterogeneity. For the Ed Yong Nature Magazine article, Biopsy Gives Only a Snapshot of Tumor Diversity, 2012, see http://www.nature.com/news/biopsy-gives-only-a-snapshot-of-tumour-diversity-1.9998.)
FUTURE - LIQUID BIOPSIES?
WILL THE FUTURE BRING LIQUID BIOPSIES, INSTEAD OF INVASIVE TUMOR BIOPSIES?
Hopefully, yes, in the future! .... According to a 2015 AACR Abstract!
In the White D et al. abstract presented at the AACR Annual Meeting in 2015, these researchers "described a method for purifying nucleic acids based on novel surface and binding chemistries" to see if liquid biopsies could be favorably compared to traditional solid tumor biopsies.
For their study, circulating cell-free DNA was purified from the plasma of seven cancer patients who had already had their surgeries. Also, DNA was purified from the cancer patients from the tissue on their slides.
Conclusion: "The two types of samples showed excellent correlation on mutations, suggesting that use of a less invasive liquid biopsy has the potential to enable actionable mutation detection without using more invasive solid tumor biopsy means." (See White D et al., Correlation of Mutations Detected in Liquid and Solid Biopsies, AACR Presentation, 2015.)
"An example of wisdom for the medical profession would be analyzing tumors for the radioactivity and immunity destroyers they contain. Then searching for the same items in the patient's environment, the water, food, cookware, and dentalware." Hulda Clark, PHD.