IMAGING
MAGNETIC RESONANCE IMAGING (MRI)
*CONSIDERING AN MRI WITH CONTRAST DYE?
With a family history of breast cancer, in 2001, Marcie Jacobs started doing screening MRIs with contrast dye (to help sharpen the image).
When she started having cognition problems, her doctors ordered a brain MRI.
She had 11 MRIs from 2001 to 2007.
Were the contrast dyes causing her cognition problems?
She sent tissue samples of her thigh and breast to be tested.
Results? Traces of gadolinium, the contrast dye, were found.
Marcie Jacobs' unabated concerns about all contrast dyes have now found her as the head of the wonderful Facebook group, Gadolinium Toxicity Illnesses. For the full story, see below.
*BREAST CANCER MRI STRATEGY
If you want to have an MRI, why not consider requesting an MRI without the contrast dye? Do note that an MRI without the dye may not be as effective, but it will definitely be safer. Please read this section for a discussion of some of the issues. It is your choice to contemplate the benefits and risks of MRIs!
If you want to have an MRI, why not consider requesting an MRI without the contrast dye? Do note that an MRI without the dye may not be as effective, but it will definitely be safer. Please read this section for a discussion of some of the issues. It is your choice to contemplate the benefits and risks of MRIs!
NOVEMBER 2019 STUDY: AFTER NORMAL MAMMOGRAMS, SUPPLEMENTAL MRIs REDUCED INTERVAL FINDINGS OF BREAST CANCER
*CAVEAT?: IT IS NOT KNOWN IF CONTRAST DYE (GADOLINIUM, ETC.) ACCOMPANIED THE MRIs. IF
SO, WEIGH THE BENEFITS AND RISKS.
We all know that extremely dense breasts are a risk factor for developing breast cancer unto itself, and dense breasts make it much more difficult to find the cancer on imaging mammograms.
Would using supplemental MRIs help in detecting breast cancer?
In the Netherlands, women with extremely dense breasts between the ages of 50 and 75 were randomly invited to have MRIs in addition to their normal mammograms. The results were that in the MRI group there were fewer interval breast cancers (interval breast cancer is cancer discovered within 12 months of the mammogram). Detecting breast cancer earlier may be helpful, but it is unclear if it is dispositive in long-term survival.
Conclusions: "The use of supplemental MRI screening in women with extremely dense breast tissue and normal results on mammography resulted in the diagnosis of significantly fewer interval cancers than mammography alone during a 2-year screening period."
(See Bakker MF et al., Supplemental MRI Screening for Women With Extremely Dense Breast Tissue, N Engl J Med, 2019)
*CAVEAT?: IT IS NOT KNOWN IF CONTRAST DYE (GADOLINIUM, ETC.) ACCOMPANIED THE MRIs. IF
SO, WEIGH THE BENEFITS AND RISKS.
We all know that extremely dense breasts are a risk factor for developing breast cancer unto itself, and dense breasts make it much more difficult to find the cancer on imaging mammograms.
Would using supplemental MRIs help in detecting breast cancer?
In the Netherlands, women with extremely dense breasts between the ages of 50 and 75 were randomly invited to have MRIs in addition to their normal mammograms. The results were that in the MRI group there were fewer interval breast cancers (interval breast cancer is cancer discovered within 12 months of the mammogram). Detecting breast cancer earlier may be helpful, but it is unclear if it is dispositive in long-term survival.
Conclusions: "The use of supplemental MRI screening in women with extremely dense breast tissue and normal results on mammography resulted in the diagnosis of significantly fewer interval cancers than mammography alone during a 2-year screening period."
(See Bakker MF et al., Supplemental MRI Screening for Women With Extremely Dense Breast Tissue, N Engl J Med, 2019)

"...Magnetic Resonance Imaging (MRI) is known to be more sensitive than mammography at detecting nearly all invasive cancers and a majority of in-situ (noninvasive) cancers. It certainly can find some tumors that mammography misses. And since MR uses a magnet to image the breast, it does not involve any radiation exposure.." Dr. Priscilla Slanetz, 2011.
"MRI is a useful adjunct to mammography for screening in high-risk women, resulting in a significantly higher rate of cancer detection. However, this was found to be at the cost of more imaging and biopsies for lesions that ultimately proved to be benign.." Raikhlin A et al., 2015..
"The study of health effects lagged far behind the commerce, so gadolinium (on MRIs) and others were injected into people to make scans more visible. When health effects did show up, it was too late.." Hulda Clark, PHD, The Cure and Prevention of All Cancers, 2007..
"MRI is a useful adjunct to mammography for screening in high-risk women, resulting in a significantly higher rate of cancer detection. However, this was found to be at the cost of more imaging and biopsies for lesions that ultimately proved to be benign.." Raikhlin A et al., 2015..
"The study of health effects lagged far behind the commerce, so gadolinium (on MRIs) and others were injected into people to make scans more visible. When health effects did show up, it was too late.." Hulda Clark, PHD, The Cure and Prevention of All Cancers, 2007..
BREAST IMAGING - MRI - WHAT IS AN MRI? - FROM THE AMERICAN CANCER SOCIETY:
"MRI scans use magnets and radio waves instead of x-rays (Note; So, no radiation) to produce very detailed, cross-sectional images of the body.
The most useful MRI exams for breast imaging use a contrast material (called gadolinium) that is injected into a catheter in a vein (IV) in the arm before or during the exam. This improves the ability of the MRI to clearly show breast tissue details.
Although MRI can find some cancers not seen on than mammogram, it is also more likely to find something that turns out not to be cancer (called a false positive). False-positive findings have to be checked out to know that cancer isn’t present, which means coming back for further tests and/or biopsies.
This is why (false positives), MRI is not recommended as a screening test for women at average risk of breast cancer, as it would result in unneeded biopsies and other tests in a large portion of these women..."
http://www.cancer.org/cancer/breastcancer/moreinformation/breastcancerearlydetection/breast-cancer-early-detection-a-c-s-recs-m-r-i.
The most useful MRI exams for breast imaging use a contrast material (called gadolinium) that is injected into a catheter in a vein (IV) in the arm before or during the exam. This improves the ability of the MRI to clearly show breast tissue details.
Although MRI can find some cancers not seen on than mammogram, it is also more likely to find something that turns out not to be cancer (called a false positive). False-positive findings have to be checked out to know that cancer isn’t present, which means coming back for further tests and/or biopsies.
This is why (false positives), MRI is not recommended as a screening test for women at average risk of breast cancer, as it would result in unneeded biopsies and other tests in a large portion of these women..."
http://www.cancer.org/cancer/breastcancer/moreinformation/breastcancerearlydetection/breast-cancer-early-detection-a-c-s-recs-m-r-i.
BREAST IMAGING - MRI - WHO SHOULD HAVE AN MRI?
Dr. Priscilla Slanetz wrote, "For the past decade, women have been undergoing breast MR to detect rupture of silicone breast implants, and this still is one of the indications.
Current data also supports its use for women who are considered to be at high risk for breast cancer (those with a greater than 20-25% lifetime risk).
In addition, selected patients with newly diagnosed breast cancer may benefit from MR preoperatively as it often can better outline the area of involvement, minimizing the need for multiple surgical procedures.
Other patients who benefit from the study include: Women with a metastatic lymph node where the primary tumor is unknown; newly diagnosed cancer patients who might be eligible for partial breast irradiation; selected patients where breast cancer recurrence is suspected clinically or on other imaging; and selected women with incompletely characterized findings on mammography and/or ultrasound. Women who are unable to undergo breast MR might include those who have pacemakers, have poor renal function, have metal in their bodies, or have allergies to the contrast agent."
(See Dr. Priscilla Slanetz, Mammogram vs MRI: Breast Screenings For High Risk Women, 2011, http://www.bidmc.org/YourHealth/Health-Notes/Medical-Imaging/Diagnostic-Tests/Mammogram-vs-MRI-Breast-Screenings-For-High-Risk-Women.aspx
BREAST IMAGING - MRI - SAFETY OF THE MRI WITH AND WITHOUT THE CONTRAST DYE, GADOLINIUM
The MRI is excellent at picking up abnormalities upon imaging, albeit with more false-positives than mammograms and ultrasounds. Dr. Priscilla Slanetz commented above that a contraindication for an MRI includes those who have "allergies to the contrast agent" given with the MRI. So, how safe is an MRI?
SAFETY OF THE MRI WITHOUT CONTRAST
The MRI does not use any radiation, making it a more favorable choice than a mammogram, especially 3D tomosynthesis. However, "The biological effects of static magnetic fields is one of the most controversial topics in the field of MR safety. It has been reported in the literature that several structures in humans are affected bt the static magnetic field, such as the retina, pineal gland, and some cells in the paranasal sinuses."
Ng K-H et al., 2003.
BUT HOW ABOUT AN MRI WITH CONTRAST DYE (ENHANCED MRI)? - POSSIBLE BRAIN HYPERINTENSITY, KIDNEY PROBLEMS CAUSING SKIN THICKENING
(SEE POSSIBLE SPECIFIC HARM FROM MULTIPLE BREAST MRIs (MARCIE JACOBS) IN NEXT SECTION.)
Breast cancer patients should be aware that a breast MRI usually involves the use of the contrast dye, gadolinium, to help sharpen to more clearly see small abnormalities. Thus, these MRIs are called "enhanced MRIs".
Brain Problems with MRI Contrast Dye? The 2014 Kanda T et al. study sought, "To explore any correlation between the number of previous gadolinium-based contrast material administrations and high signal intensity in the dentate nucleus and globus pallidus ..." For their study, people with six or more MRIs with contrast dye were compared with people who had six or fewer MRIs without the dye. The brain testing revealed that there was hypersensitivity in two parts of the brain in the people who had multiples MRIs with contrast dye.
These results, Dr. Joseph Mercola commented, "revealed areas of high intensity, or hyperintensity, in two brain regions (the dentate nucleus (DN) and globus pallidus (GP)), which correlated with the number of gadolinium-based enhanced MRIs. It’s unknown at this time what the hyperintensity may mean, however hyperintensity in the DN is associated with multiple sclerosis. It’s now being suggested that this hyperintensity may be the result of the large number of enhanced MRI scans often received by multiple sclerosis patients. Hyperintensity of the GP, meanwhile, is linked with liver dysfunction. The study’s lead author noted, 'Hyperintensity in the dentate nucleus and globus pallidus on unenhanced MRI may be a consequence of the number of previous Gd-CM administrations… Because gadolinium has a high signal intensity in the body, our data may suggest that the toxic gadolinium component remains in the body even in patients with normal renal function.' " (Dr. Mercola, 2014.)
Kidney Problems with MRI Contrast Dye? From Dr. Mercola: "Among patients with severe kidney disease, the use of gadolinium-based contrast agents is linked to the development of Nephrogenic Systemic Fibrosis, or NSF. NSF was first identified in 1997 and while its cause is unknown, it’s only been reported in those with kidney disease. NSF causes skin thickening that can prevent bending and extending your joints. It can also develop in your diaphragm, thigh muscles, lung vessels, and lower abdomen. Along with causing decreased mobility of joints, NSF can be fatal."
(For the Ng safety study, Ng K-H et al.,Magnetic Research Imagining, Health Effects and Safety,Proceedings of the International Conference on Non-Ionizing Radiation at UNITEN. Electromagnetic Fields and Our Health , 2003http://www.who.int/peh-emf/meetings/archive/en/paper04ng.pdf. For the Kanda brain study, Kanda T et al., High Signal Intensity in the Dentate Nucleus and Globus Pallidus on Unenhanced T1-Weight MR Images: Relationship with Increasing Cumulative Dose of Gadolinium-Based Contrast Medium, Radiology, 2014. For Dr. Mercola's 2014 comments, Gadolinium: The MRI Agent Linked to Brain Abnormalities, http://articles.mercola.com/sites/articles/archive/2014/01/09/gadolinium-mri-contrast-agent.aspx#_edn4, )
Brain Problems with MRI Contrast Dye? The 2014 Kanda T et al. study sought, "To explore any correlation between the number of previous gadolinium-based contrast material administrations and high signal intensity in the dentate nucleus and globus pallidus ..." For their study, people with six or more MRIs with contrast dye were compared with people who had six or fewer MRIs without the dye. The brain testing revealed that there was hypersensitivity in two parts of the brain in the people who had multiples MRIs with contrast dye.
These results, Dr. Joseph Mercola commented, "revealed areas of high intensity, or hyperintensity, in two brain regions (the dentate nucleus (DN) and globus pallidus (GP)), which correlated with the number of gadolinium-based enhanced MRIs. It’s unknown at this time what the hyperintensity may mean, however hyperintensity in the DN is associated with multiple sclerosis. It’s now being suggested that this hyperintensity may be the result of the large number of enhanced MRI scans often received by multiple sclerosis patients. Hyperintensity of the GP, meanwhile, is linked with liver dysfunction. The study’s lead author noted, 'Hyperintensity in the dentate nucleus and globus pallidus on unenhanced MRI may be a consequence of the number of previous Gd-CM administrations… Because gadolinium has a high signal intensity in the body, our data may suggest that the toxic gadolinium component remains in the body even in patients with normal renal function.' " (Dr. Mercola, 2014.)
Kidney Problems with MRI Contrast Dye? From Dr. Mercola: "Among patients with severe kidney disease, the use of gadolinium-based contrast agents is linked to the development of Nephrogenic Systemic Fibrosis, or NSF. NSF was first identified in 1997 and while its cause is unknown, it’s only been reported in those with kidney disease. NSF causes skin thickening that can prevent bending and extending your joints. It can also develop in your diaphragm, thigh muscles, lung vessels, and lower abdomen. Along with causing decreased mobility of joints, NSF can be fatal."
(For the Ng safety study, Ng K-H et al.,Magnetic Research Imagining, Health Effects and Safety,Proceedings of the International Conference on Non-Ionizing Radiation at UNITEN. Electromagnetic Fields and Our Health , 2003http://www.who.int/peh-emf/meetings/archive/en/paper04ng.pdf. For the Kanda brain study, Kanda T et al., High Signal Intensity in the Dentate Nucleus and Globus Pallidus on Unenhanced T1-Weight MR Images: Relationship with Increasing Cumulative Dose of Gadolinium-Based Contrast Medium, Radiology, 2014. For Dr. Mercola's 2014 comments, Gadolinium: The MRI Agent Linked to Brain Abnormalities, http://articles.mercola.com/sites/articles/archive/2014/01/09/gadolinium-mri-contrast-agent.aspx#_edn4, )
SAFETY OF MRI WITH DYE?
MARCIE JACOBS - MAY MULTIPLE BREAST MRIs WITH DYE CAUSE HARM?
When she (Marcie Jacobs) started having problems, being sick from these MRIs, her doctors ordered - you guessed it - a brain MRI with contrast dye to see what was the matter!
Quite possibly .... Harm that is described in Jeff Gerth's wonderful 2015 article on MRIs and dye.
Jeff Gerth characterized possible problems that may be associated with MRIs with gadolinium -containing contrast dye. Specifically, in the article, for one woman, horrific problems ensued following multiple breast MRIs with dye.
"With a family history of breast cancer, Marcie Jacobs decided in June 2001 that an MRI screening was her best preventive option. As is common with MRIs, Jacobs was injected beforehand with a contrast agent, a drug that helps sharpen the resulting images. But after a few of these treatments, she began noticing some strange cognitive effects. Jacobs began missing meetings. Over the next several years she had additional MRIs. The math skills that were crucial to her job as finance manager started deteriorating, she said. Jacobs eventually wound up on disability."
Any clues to what was causing her problems? "Jacobs has no medical proof, but she’s convinced the two drugs (Omniscan and Magnevist) are behind her problems. ...She recovered old records and determined that she received Omniscan for her first 11 imagings and Magnevist before the last, in 2007. ... She stopped worrying about cancer – and started worrying about imaging drugs.."
Proof? When she started having problems, being sick from these MRIs, her doctors ordered - you guessed it - a brain MRI with contrast dye to see what was the matter! The brain MRI showed high signal intensity, conforming with the hypersensitivity found from MRIs with gadolinium in the Kanda study (see the section above). She was so determined to find out if the dyes were a problem that she actually sent tissue samples taken from the thigh and the breast to be tested. Results? The thigh and breast samples did show traces of gadolinium, which illustrates that there is gadolinium retention. In addition, via testing, she discovered that she has fatty degeneration of the liver, a finding now coming to light. For all of these problems, needless to say, "Doctors were puzzled because she had no history of kidney disease and did not fit into the identified at-risk group."
Jeff Gerth characterized possible problems that may be associated with MRIs with gadolinium -containing contrast dye. Specifically, in the article, for one woman, horrific problems ensued following multiple breast MRIs with dye.
"With a family history of breast cancer, Marcie Jacobs decided in June 2001 that an MRI screening was her best preventive option. As is common with MRIs, Jacobs was injected beforehand with a contrast agent, a drug that helps sharpen the resulting images. But after a few of these treatments, she began noticing some strange cognitive effects. Jacobs began missing meetings. Over the next several years she had additional MRIs. The math skills that were crucial to her job as finance manager started deteriorating, she said. Jacobs eventually wound up on disability."
Any clues to what was causing her problems? "Jacobs has no medical proof, but she’s convinced the two drugs (Omniscan and Magnevist) are behind her problems. ...She recovered old records and determined that she received Omniscan for her first 11 imagings and Magnevist before the last, in 2007. ... She stopped worrying about cancer – and started worrying about imaging drugs.."
Proof? When she started having problems, being sick from these MRIs, her doctors ordered - you guessed it - a brain MRI with contrast dye to see what was the matter! The brain MRI showed high signal intensity, conforming with the hypersensitivity found from MRIs with gadolinium in the Kanda study (see the section above). She was so determined to find out if the dyes were a problem that she actually sent tissue samples taken from the thigh and the breast to be tested. Results? The thigh and breast samples did show traces of gadolinium, which illustrates that there is gadolinium retention. In addition, via testing, she discovered that she has fatty degeneration of the liver, a finding now coming to light. For all of these problems, needless to say, "Doctors were puzzled because she had no history of kidney disease and did not fit into the identified at-risk group."
It was always believed, and the belief was well-disseminated, that these contrast dyes were harmlessly excreted from the body. Through the hard way, Marcie Jacobs discovered otherwise.
Marcie Jacobs started a Facebook page, Gadolinium Toxicity Illnesses! Go to: https://www.facebook.com/groups/Gadolinium/?fref=nf. One of our Editors is a member. Join the discussion! (For the article, see Jeff Gerth, Left in the Brain: Potentially Toxic Residue from MRI Drugs, ProPublica, 2015,https://www.propublica.org/article/left-in-the-brain-potentially-toxic-residue-from-mri-drugs.)
SO, YOU GO AHEAD AND HAVE AN MRI WITH CONTRAST DYE - ANY WAY TO AMELIORATE THE DAMAGE OF THE DYES? - A FEW IDEAS
1. After the MRI imaging test with contrast dye, drink lots of water to try to flush out gadolinium.
2. For gadolinium retention, consider some kind of chelation therapy. Consult a medical professional. From Jeff Gerth's article, "Marcie Jacobs said she eventually began a difficult, extended program to remove gadolinium from her body."
3. Right after the test, consider magnets. Dr. Clark believed that gadolinium, a lanthanide, could not be separated from other lanthanides and were all together in contrast materials. Early on, Dr. Clark recommended using a TINY magnet (not over 100 gauss). "The magnet should be placed lengthwise over the center-line that you draw along your spine. The back of your neck is convenient. THE NORTH SIDE OF THE PATCH IS PLACED AGAINST THE SKIN AND HELD THERE WITH MASKING TAPE. The main purpose of the small magnet is to pull iron and lanthanides out of your tissues; this includes excess ferritin that coats your white blood cells." NOTE: IN LATER YEARS, DR. CLARK WAS WORRIED ABOUT THE IMPROPER USE OF THE MAGNETS, AND WAS RETICENT TO RECOMMEND THEM. From www.drclark.net, "Mistaken polarity helps bacteria and fungi grow! If uncertain, do not use them (the magnets)!"
4. How about N-acetyl-cysteine? In the Pereira L et al. 2012 study, the researchers "evaluated the effect of Gadonium-chelate on renal function, iron parameters and oxidative stress in rats with chronic renal failure and a possible protective effect of the antioxidant, N-acetylcysteine. In the rats, a pre-treatment of N-acetyl cysteine two days before gadolinium administration, and N-acetylcysteine maintained during four days "suggest that cysteine can prevent gadolinium-chelate nephrotoxicity in patients with chronic renal failure." Thus, "The antioxidant effect of cysteine can prevent gadolinium toxicity and even the development of nephrogenic systemic fibrosis."
(See Pereira L et al., N-Acetyl Cysteine Protects Rats with Chronic Renal Failure from Gadolinium-Chelate Nephrotoxicity, PLOS One, 2012.)
2. For gadolinium retention, consider some kind of chelation therapy. Consult a medical professional. From Jeff Gerth's article, "Marcie Jacobs said she eventually began a difficult, extended program to remove gadolinium from her body."
3. Right after the test, consider magnets. Dr. Clark believed that gadolinium, a lanthanide, could not be separated from other lanthanides and were all together in contrast materials. Early on, Dr. Clark recommended using a TINY magnet (not over 100 gauss). "The magnet should be placed lengthwise over the center-line that you draw along your spine. The back of your neck is convenient. THE NORTH SIDE OF THE PATCH IS PLACED AGAINST THE SKIN AND HELD THERE WITH MASKING TAPE. The main purpose of the small magnet is to pull iron and lanthanides out of your tissues; this includes excess ferritin that coats your white blood cells." NOTE: IN LATER YEARS, DR. CLARK WAS WORRIED ABOUT THE IMPROPER USE OF THE MAGNETS, AND WAS RETICENT TO RECOMMEND THEM. From www.drclark.net, "Mistaken polarity helps bacteria and fungi grow! If uncertain, do not use them (the magnets)!"
4. How about N-acetyl-cysteine? In the Pereira L et al. 2012 study, the researchers "evaluated the effect of Gadonium-chelate on renal function, iron parameters and oxidative stress in rats with chronic renal failure and a possible protective effect of the antioxidant, N-acetylcysteine. In the rats, a pre-treatment of N-acetyl cysteine two days before gadolinium administration, and N-acetylcysteine maintained during four days "suggest that cysteine can prevent gadolinium-chelate nephrotoxicity in patients with chronic renal failure." Thus, "The antioxidant effect of cysteine can prevent gadolinium toxicity and even the development of nephrogenic systemic fibrosis."
(See Pereira L et al., N-Acetyl Cysteine Protects Rats with Chronic Renal Failure from Gadolinium-Chelate Nephrotoxicity, PLOS One, 2012.)
To reiterate, if you want to have an MRI, why not consider requesting an MRI without the contrast dye? Do note that an MRI without the dye may not be as effective, but it will definitely be safer. It is your choice to contemplate the benefits and risks!
BREAST IMAGING - MRI
BREAST MRI IMPROVES DETECTION OF INVASIVE CANCERS, PREINVASIVE CANCERS, AND PREMALIGNANT LESIONS IN HIGH RISK WOMEN
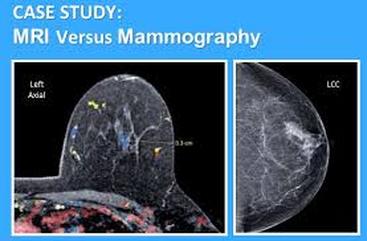
"The same breast, imaged by MRI (left) and mammography (right). Mammography misses operable, precancerous growths — in this case, early surgery based on MRI screening could prevent breast cancer."
In the Riedl C et al 2007 study, the researchers posited that the "high false-positive rate" in their study was "partially caused by an unusually high number of the lesions" - atypical ductal hyperplasia.
Indeed, the researchers asserted that MRI improves the detection of invasive cancers, preinvasive cancers, and premalignant lesions", and should be used in a "high-risk population for breast cancer.
Indeed, the researchers asserted that MRI improves the detection of invasive cancers, preinvasive cancers, and premalignant lesions", and should be used in a "high-risk population for breast cancer.
In the Riedl C et al. 2007 study , the researchers evaluated mammography, ultrasound, and MRI relative to women at high risk for breast cancer.
Results: 327 women completed 672 rounds of imaging. "Of a total of 28 detected cancers, 14 were detected by mammography, 12 by ultrasound, and 24 by MRI, which resulted in sensitivities of 50%, 42.9%, and 85.7%, respectively. MRI detected not only significantly more invasive but also significantly more preinvasive cancers (ductal carcinoma in situ). Mammography, ultrasound, and MRI led to 25, 26, and 101 false-positive findings, which resulted in specificities of 98%, 98%, and 92%, respectively. Thirty-five (35%) of these false-positive findings were atypical ductal hyperplasias, lesions considered to be of premalignant character. Nine (26%) of those were detected by mammography, 2 (6%) with ultrasound, and 32 (91%) with MRI.
A criticism of MRIs is that too many false-positives are found.
The researchers counter: "The high false-positive rate in this study was partially caused by an unusually high number of detected lesions classified as ADH (atypical ductal hyperplasia).
These lesions constituted 35% of all benign findings, and the majority of the lesions were detected by MRI. For an initial statistical analysis of the diagnostic variables, we considered ADH as a benign result because this is the widely accepted approach when analyzing breast surveillance studies. However, recent studies that compared benign tissue, ADH, DCIS, and invasive cancer, using mRNA expression profiling, quantitative real-time PCR analysis, and analysis of allelic imbalance, showed that ADH is a genetically advanced precancerous lesion and that ADH, similar to DCIS, is a nonobligatory direct precursor of invasive ductal cancer."
Conclusion: "Our results show that MRI of the breast improves the detection of invasive cancers, preinvasive cancers, and premalignant lesions in a high-risk population and should therefore become an integral part of breast cancer surveillance in these patients."
More specifically, "The results of this study suggest that MRI of the breast improves detection not only of invasive malignant lesions but also of preinvasive lesions (DCIS) and premalignant lesions (e.g. ADH ) at surveillance of women with a high risk for breast cancer. It is the detection of such early-stage cancers that screening programs aim for because the rationale of an alleged long-term benefit of breast cancer surveillance is that lesions are detected in stages that still allow curative therapy. Further, the detection of preinvasive and premalignant lesions could have major implications in an individual's risk assessment and further patient management. MRI should therefore become an integral part of breast cancer surveillance in these patients. That such measures will have a positive effect, in terms of saved years of life, seems reasonable to extrapolate but remains unproven."
(See Riedl C et al., Magnetic Resonance Imaging of the Breast Improves Detection of Invasive Cancer, Preinvasive Cancer, and Premalignant Lesions During Surveillance of Women at High Risk for Breast Cancer, Clinical Cancer Reserach, 2007.)
Results: 327 women completed 672 rounds of imaging. "Of a total of 28 detected cancers, 14 were detected by mammography, 12 by ultrasound, and 24 by MRI, which resulted in sensitivities of 50%, 42.9%, and 85.7%, respectively. MRI detected not only significantly more invasive but also significantly more preinvasive cancers (ductal carcinoma in situ). Mammography, ultrasound, and MRI led to 25, 26, and 101 false-positive findings, which resulted in specificities of 98%, 98%, and 92%, respectively. Thirty-five (35%) of these false-positive findings were atypical ductal hyperplasias, lesions considered to be of premalignant character. Nine (26%) of those were detected by mammography, 2 (6%) with ultrasound, and 32 (91%) with MRI.
A criticism of MRIs is that too many false-positives are found.
The researchers counter: "The high false-positive rate in this study was partially caused by an unusually high number of detected lesions classified as ADH (atypical ductal hyperplasia).
These lesions constituted 35% of all benign findings, and the majority of the lesions were detected by MRI. For an initial statistical analysis of the diagnostic variables, we considered ADH as a benign result because this is the widely accepted approach when analyzing breast surveillance studies. However, recent studies that compared benign tissue, ADH, DCIS, and invasive cancer, using mRNA expression profiling, quantitative real-time PCR analysis, and analysis of allelic imbalance, showed that ADH is a genetically advanced precancerous lesion and that ADH, similar to DCIS, is a nonobligatory direct precursor of invasive ductal cancer."
Conclusion: "Our results show that MRI of the breast improves the detection of invasive cancers, preinvasive cancers, and premalignant lesions in a high-risk population and should therefore become an integral part of breast cancer surveillance in these patients."
More specifically, "The results of this study suggest that MRI of the breast improves detection not only of invasive malignant lesions but also of preinvasive lesions (DCIS) and premalignant lesions (e.g. ADH ) at surveillance of women with a high risk for breast cancer. It is the detection of such early-stage cancers that screening programs aim for because the rationale of an alleged long-term benefit of breast cancer surveillance is that lesions are detected in stages that still allow curative therapy. Further, the detection of preinvasive and premalignant lesions could have major implications in an individual's risk assessment and further patient management. MRI should therefore become an integral part of breast cancer surveillance in these patients. That such measures will have a positive effect, in terms of saved years of life, seems reasonable to extrapolate but remains unproven."
(See Riedl C et al., Magnetic Resonance Imaging of the Breast Improves Detection of Invasive Cancer, Preinvasive Cancer, and Premalignant Lesions During Surveillance of Women at High Risk for Breast Cancer, Clinical Cancer Reserach, 2007.)
BREAST IMAGING - MRI
FAMILIAL RISK OF BREAST CANCER? - MAMMOGRAMS OR MAMMOGRAMS COMBINED WITH ULTRASOUND - NOT AS EFFECTIVE AS MRI IN DIAGNOSIS TO FIND THINGS AT AN EARLIER, MORE FAVORABLE STAGE
Have a family history of breast cancer? With or without BRCA mutations?
In accord with the Riedl study above, the Kuhl CK et al 2005 study stated that, "If MRI is used for surveillance, then diagnosis of intraductal and invasive familial or hereditary cancer is achieved with a significantly higher sensitivity and at a more favorable stage."
In accord with the Riedl study above, the Kuhl CK et al 2005 study stated that, "If MRI is used for surveillance, then diagnosis of intraductal and invasive familial or hereditary cancer is achieved with a significantly higher sensitivity and at a more favorable stage."
In the Kuhl CK et al. study, the researchers compared mammograms, ultrasounds, and MRIs in women who had a familial risk of 20% or more to get breast cancer.
In their study, 529 asymptomatic women were given annual imaging exams in different combinations and followed for 5.3 years.
Results: Of the tumors found, "In the analysis by modality, sensitivity was low for mammography (33%) and ultrasound (40%) or the combination of both (49%). MRI offered a significantly higher sensitivity (91%)."
Conclusion: "Mammography alone, and also mammography combined with breast ultrasound, seems insufficient for early diagnosis of breast cancer in women who are at increased familial risk with or without documented BRCA mutation. If MRI is used for surveillance, diagnosis of intraductal and invasive familial or hereditary cancer is achieved with a significantly higher sensitivity and at a more favorable stage."
(See Kuhl CK et al., Mammography, Breast Ultrasound, and Magnetic Resonance Imaging for Surveillance of Women at High Familial Risk for Breast Cancer, J Clin Oncol, 2005.)
In their study, 529 asymptomatic women were given annual imaging exams in different combinations and followed for 5.3 years.
Results: Of the tumors found, "In the analysis by modality, sensitivity was low for mammography (33%) and ultrasound (40%) or the combination of both (49%). MRI offered a significantly higher sensitivity (91%)."
Conclusion: "Mammography alone, and also mammography combined with breast ultrasound, seems insufficient for early diagnosis of breast cancer in women who are at increased familial risk with or without documented BRCA mutation. If MRI is used for surveillance, diagnosis of intraductal and invasive familial or hereditary cancer is achieved with a significantly higher sensitivity and at a more favorable stage."
(See Kuhl CK et al., Mammography, Breast Ultrasound, and Magnetic Resonance Imaging for Surveillance of Women at High Familial Risk for Breast Cancer, J Clin Oncol, 2005.)
BREAST IMAGING - MRI
ANY PROBLEMS? 2015 STUDY - MRI HAS "SIGNIFICANTLY" HIGHER RATE OF BREAST CANCER DETECTION, BUT.... MORE FALSE POSITIVES, LEADING TO MORE IMAGING, BIOPSIES FOR BENIGN FINDINGS
In the Raikhlin A et al 2015 study, MRI had a "significantly higher rate of cancer detection. However, this was found to be at the cost of more imaging and biopsies for lesions that ultimately proved to be benign."
In the 2015 Raikhlin A et al. study, the researchers assessed mammograms and MRIs for their screening efficacy in women who were at high risk for breast cancer.
Results: " Malignancy was diagnosed (out of 650 high-rsik women)in 13 patients (invasive cancer in nine, ductal carcinoma in situ in three [one with microinvasion], and chest wall metastasis in one). Of the 13 cancers, 12 (92.3%) were detected by MRI and four (30.8%) by mammography. In nine of these patients, the cancer was diagnosed by MRI only, resulting in an incremental cancer detection rate of 10 cancers per 1000 women screened. MRI screening had significantly higher sensitivity than mammography (92.3% vs 30.8%) but lower specificity (85.9% vs 96.8%). MRI also resulted in a higher callback rate for a 6-month follow-up study (BI-RADS category 3 assessment) than mammography (119 [14.8%] vs 13 [1.6%]) and more image-guided biopsies than mammography (95 -11.8% vs 19 - 2.4%."
Conclusion: "MRI is a useful adjunct to mammography for screening in high-risk women, resulting in a significantly higher rate of cancer detection. However, this was found to be at the cost of more imaging and biopsies for lesions that ultimately proved to be benign."
(See Raikhlin A et al., Breast MRI as an Adjunct to Mammography for Breast Cancer Screening in High-Risk Patients: Retrospective Review, American Journal of Roentgenology, 2015.)
BREAST IMAGING - MRI - ANY PROBLEMS? 2015 STUDY - NOT JUST FALSE-POSITIVES IN BREAST, BUT OUTSIDE OF THE BREAST, TOO!!
INCIDENTAL FINDINGS ON MRI
TOTAL STATISTICS
NO 292 89.3
YES 35 10.7
TOTAL STATISTICS
NO 292 89.3
YES 35 10.7
* FALSE-POSITIVES IN THE BREAST
* FALSE-POSITIVES OUTSIDE OF BREAST, TOO?
On MRI testing, extra-mammary (outside the breast) findings were reported in 10.7% of the patients - namely, 35 out of 327 patients, totaling 38 "incidental findings". Specifically, 21 findings in the liver, 12 in the thoracic cavity, 1 in the kidneys, 3 in the musculoskeletal system, and 1 in the neck. These findings resulted in 18 of the 35 patients with these findings being referred to doctors, and two had a biopsy.
Although 10.7% of the breast cancer patients who had MRIs were found to have incidental extra-mammary findings, none had any other cancer.
PAdia SA et al., 2015
* FALSE-POSITIVES OUTSIDE OF BREAST, TOO?
On MRI testing, extra-mammary (outside the breast) findings were reported in 10.7% of the patients - namely, 35 out of 327 patients, totaling 38 "incidental findings". Specifically, 21 findings in the liver, 12 in the thoracic cavity, 1 in the kidneys, 3 in the musculoskeletal system, and 1 in the neck. These findings resulted in 18 of the 35 patients with these findings being referred to doctors, and two had a biopsy.
Although 10.7% of the breast cancer patients who had MRIs were found to have incidental extra-mammary findings, none had any other cancer.
PAdia SA et al., 2015
As illustrated in this IMAGING-MRI section, MRI has been shown to have "a high false-positive rate for additional findings in the breast resulting in additional breast imaging and biopsies.".
How about outside the breast?
In the 2015 Padia SA et al. study, the researchers "hypothesized that breast MRI is also associated with a high rate of false-positive findings outside of the breast requiring additional evaluation, interventions, and delays in treatment."
Examining the records of 327 breast cancer patients who had breast MRIs, it was discovered that extra-mammary (outside the breast) findings were reported in 10.7% of the patients - namely, 35 out of 327 patients, totaling 38 "incidental findings". Specifically, 21 findings in the liver, 12 in the thoracic cavity, 1 in the kidneys, 3 in the musculoskeletal system, and 1 in the neck. These findings resulted in 18 of the 35 patients with these findings being referred to doctors, and two had a biopsy.
Results: Although 10.7% of the breast cancer patients who had MRIs were found to have incidental extra-mammary findings, none had any other cancer.
Conclusion: "Extra-mammary findings highlight an unrecognized adverse consequence of breast MRI."
(See Padia SA, False-Positive Extra-Mammary Findings in Breast MRI: Another Cause for Concern, Breast J, 2015.)
How about outside the breast?
In the 2015 Padia SA et al. study, the researchers "hypothesized that breast MRI is also associated with a high rate of false-positive findings outside of the breast requiring additional evaluation, interventions, and delays in treatment."
Examining the records of 327 breast cancer patients who had breast MRIs, it was discovered that extra-mammary (outside the breast) findings were reported in 10.7% of the patients - namely, 35 out of 327 patients, totaling 38 "incidental findings". Specifically, 21 findings in the liver, 12 in the thoracic cavity, 1 in the kidneys, 3 in the musculoskeletal system, and 1 in the neck. These findings resulted in 18 of the 35 patients with these findings being referred to doctors, and two had a biopsy.
Results: Although 10.7% of the breast cancer patients who had MRIs were found to have incidental extra-mammary findings, none had any other cancer.
Conclusion: "Extra-mammary findings highlight an unrecognized adverse consequence of breast MRI."
(See Padia SA, False-Positive Extra-Mammary Findings in Breast MRI: Another Cause for Concern, Breast J, 2015.)